

Overview of oxygen sources
Contributors: Sky Vanderburg, Michael Lipnick, MD, Robert Neighbour, Cornelius Sendagire, MMed
Date last updated: Aug 15, 2024
This article will review the four most common sources of medical oxygen: oxygen cylinders, oxygen concentrators, oxygen plants, and liquid oxygen. While historically, liquid oxygen (LOX) has been relatively more common only in well-resourced settings, in the wake of the SARS-CoV-2 pandemic, significant efforts were set in motion to scale up access to LOX as well as other oxygen supply types in resource-limited settings, too.
Medical grade oxygen must be >82% purity and without contamination. Oxygen used at clinical sites is either: 1) generated offsite and transported via cylinders in gaseous or liquid form; or 2) generated onsite via oxygen concentrators or plants. Oxygen is then delivered to patients via wall medical gas piping—either directly from an onsite oxygen plant or from a manifold supplied by oxygen cylinders—or via oxygen cylinders or concentrators placed at the bedside.
Here we refer to oxygen sources as low, intermediate and high pressure:
- “Low pressure” – < 2bar/20 PSI
- “Intermediate pressure” – 3.4bar/55PSI
- “High pressure” – >137bar/2000PSI
Choosing the optimal oxygen supply setup can be challenging and limited data exist to guide cost-effectiveness. This article discusses the different sources of medical oxygen, including advantages and disadvantages of each source.
Always consult the manufacturer’s specifications and recommendations prior to using any oxygen sources. Improper use or ‘DIY’ approaches can be dangerous. In most countries, parts must comply with national regulatory body standards.
An overview of oxygen delivery devices and oxygen connector types can be found elsewhere in this O2 Encyclopedia.
Oxygen Cylinders
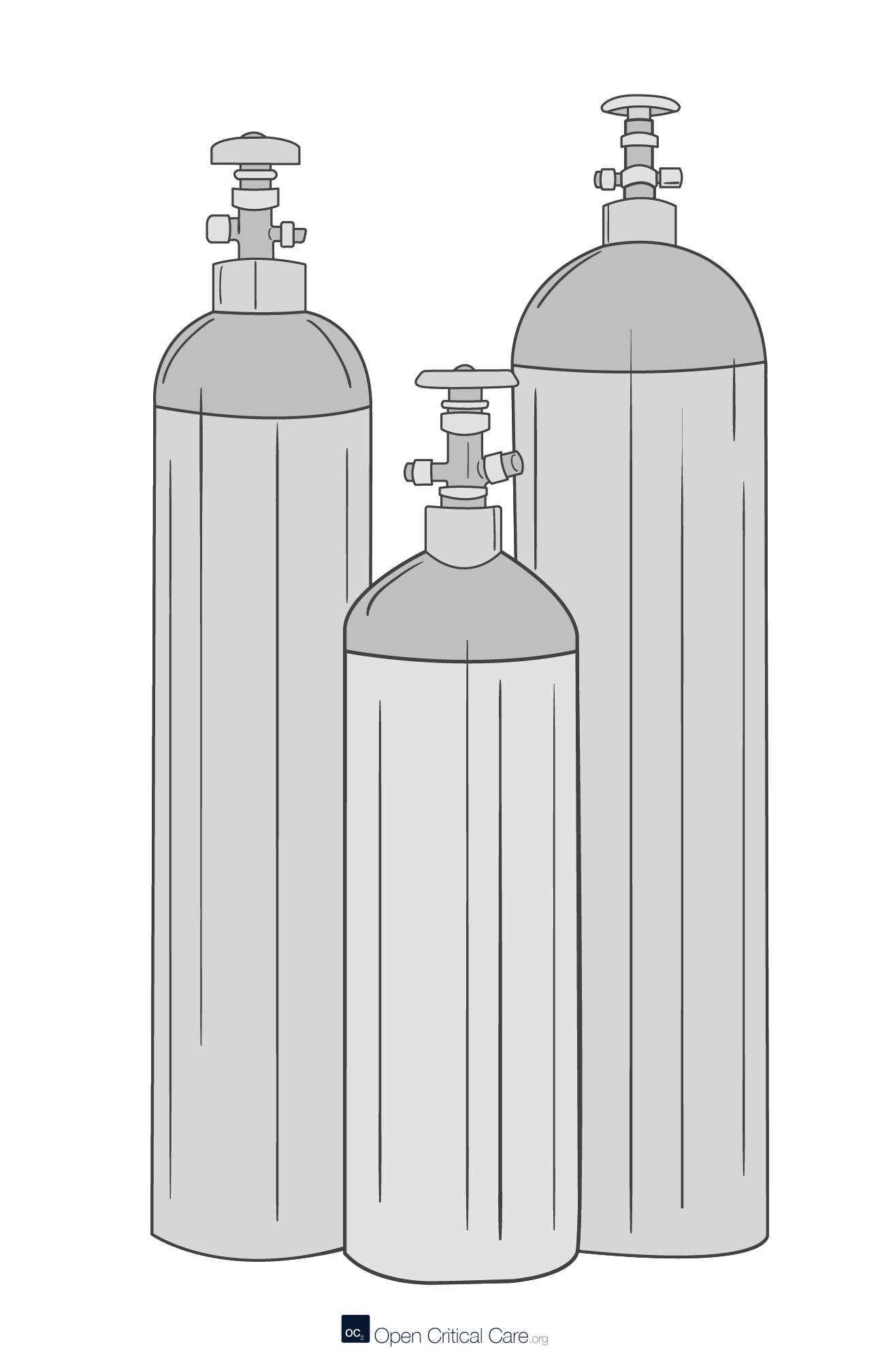
Oxygen Cylinders
- O2 concentration: varies depending on type and quality of source (e.g. 99.9% if filled from LOX; 94% if filled from PSA; <80% if low quality source)
- Distribution: can be placed at the bedside (secured) or connected to a manifold pipeline distribution system
- Capacity: wide range of sizes ranging from 100-10,000L (gaseous) capacity (Cylinder size and duration calculator)
- Pressure: if filled then can provide high (2000psi, 137bar) or intermediate pressure (50psi, 4bar via regulator) oxygen to delivery devices that require such pressure to operate; should be refilled if residual pressure < ~ 29psi (2 bar, 200kPa) to prevent ingress of contaminants including moisture.
- Costs: moderate cost (e.g. $60-$250 “J” 6800L cylinder) for the cylinder though also require regulator, flowmeter, and delivery; ongoing costs can be high including cylinder deposit or leasing fee, refill costs (e.g. $25-$100 per “J” cylinder) and transport costs.
- Advantages: portable, common, can be used at facilities without O2 piping systems, do not require power, easy to use
- Disadvantages: large cylinders are heavy, require special facilities to refill (often not available at hospitals), exhaustible supply, easy relocation to unintended places, can be safety hazard if not properly secured and maintained
Always store oxygen cylinders with safety cap.
Portable Oxygen Concentrators (PSA)

Portable Oxygen Concentrators (PSA)
- O2 concentration: if functioning properly, then 92-96%
- Distribution: most small units can be placed at the bedside and connected directly to the patient, or placed near the patient area
- Capacity: wide range of outputs, most commonly 3-10 L/min, though some portable units may produce 30-50 LPM (Oxygen concentrator supply calculator)
- Pressure: most units provide low pressure only (this is far less than the 50psi/4bar needed to run HFNC, and most ventilators and NIPPV devices)
- Costs: moderate cost for the unit (USD$500-2000 depending on output 3-10LPM)
- Advantages: portable, common, can be used at facilities without O2 piping, easy to use, inexhaustible supply
- Disadvantages: require continuous power (350-600W, not variable with flows), easy relocation to unintended places, low pressure output, requires some maintenance, can be loud in patient care spaces
Oxygen Plants (PSA/VSA/VPSA)
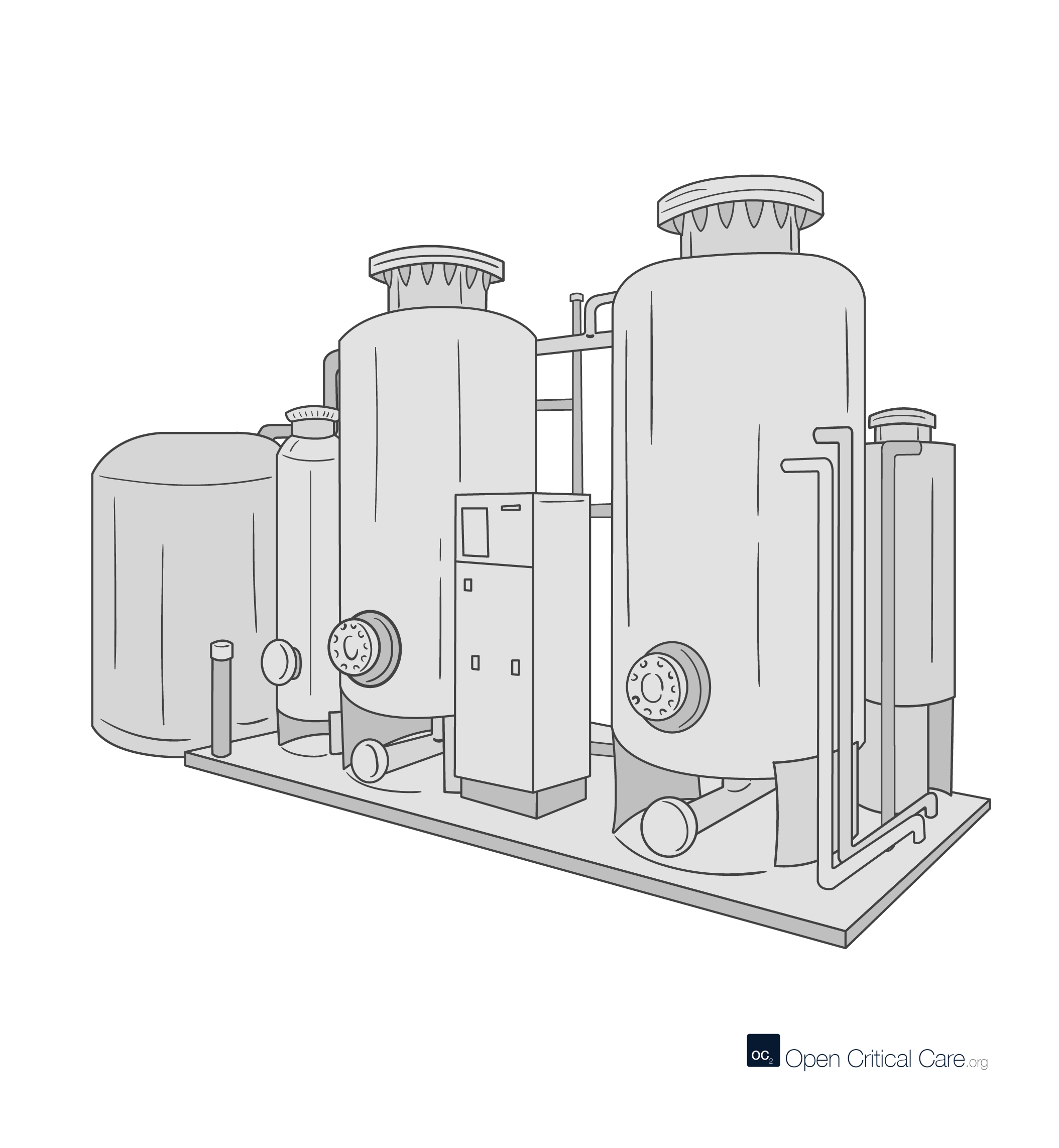
Oxygen Plants (PSA/VSA/VPSA)
- O2 concentration: 93% ± 3, though concentration can drop <80% for overtaxed or malfunctioning plants
- Distribution: Stationary. Can be installed at clinical site with oxygen delivered to patient care areas via medical gas piping systems or cylinders
- Capacity: wide range of flows depending on manufacturer specifications (0.5 – 200 Nm3/hr) (8-2,500 liters per minute) (VSA plants 50-3,100 Nm3/hr at 5 psig)
- Pressure: Output is intermediate pressure oxygen (3-6 bar) which is either delivered directly via medical gas piping systems (3-6 bar) or compressed further (~137 bar) to fill oxygen cylinders.
- Costs: high initial costs for installation and infrastructure, though ongoing costs can be low
- Advantages: continuous supply; can have relatively low ongoing costs, designed for 10 year minimum lifespan
- Disadvantages: requires continuous supply of electricity (~1.2kWh per m^3 flow), high initial costs, requires regular skilled maintenance
Liquid Oxygen (LOX)
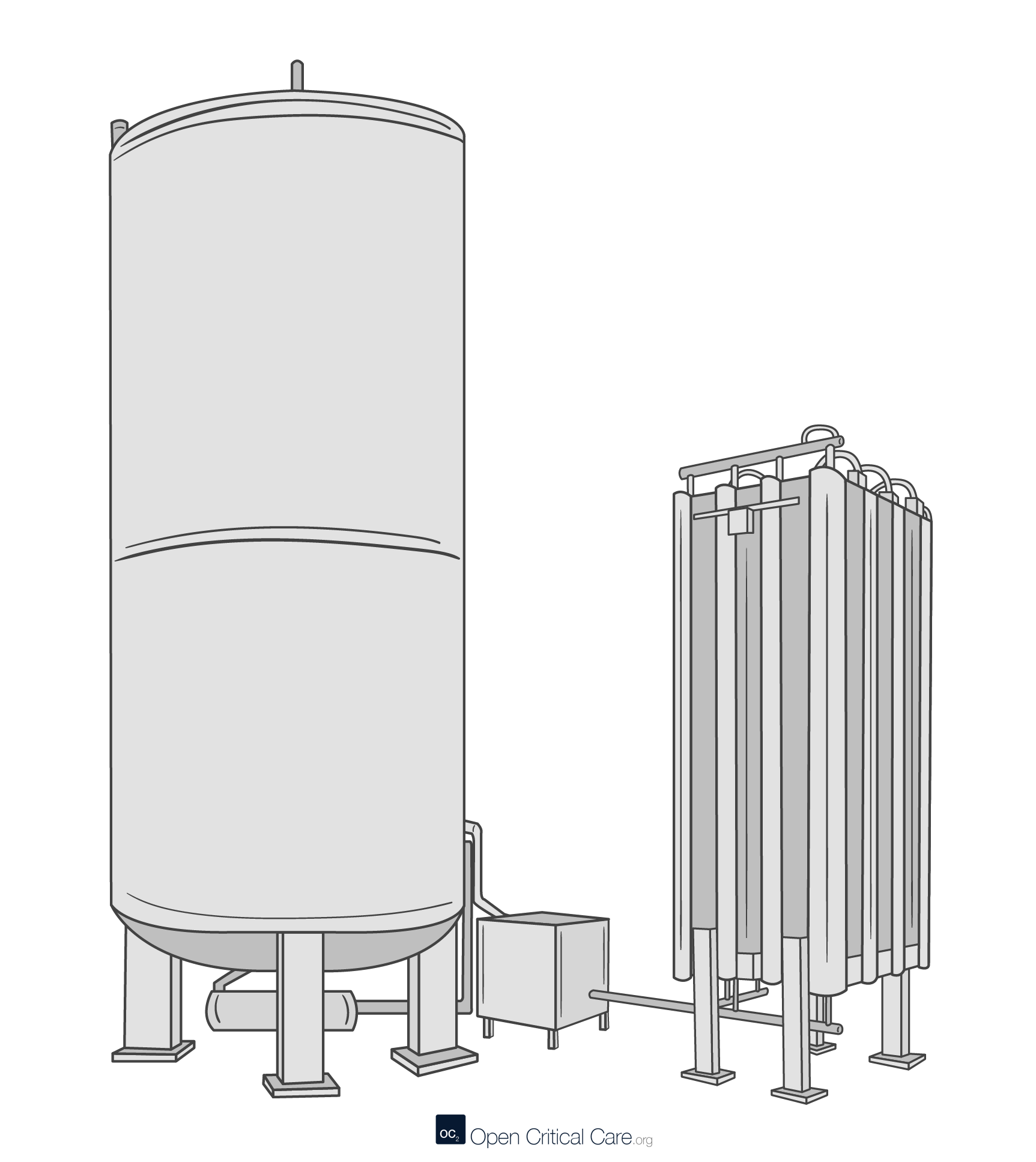
Liquid Oxygen (LOX)
- O2 concentration: highest purity medical oxygen concentration ~99.5%
- Distribution: Stationary. LOX is generated at Air Separation Units (ASUs) and must be transported by certified tanker truck from the ASU to the healthcare facility where it is stored and released to the hospital thru vacuum insulated evaporators (VIE). O2 then delivered to patient care areas via wall piping or cylinders.
- Capacity: storage tanks can hold 500-25,000 liquid liters of oxygen (i.e. up to 21,500,000 gaseous liters); flow output varies by VIE design and commonly ranges 150-20,000 gaseous liters per minute.
- Pressure: Output from a VIE is >3-6 bar and must be pressure regulated to (3-6 bar) for delivery directly via medical gas piping systems (3-6 bar) or can be compressed further (~137 bar) to fill oxygen cylinders.
- Costs: intermediate initial costs for installation and infrastructure for the VIE ($10,000 to $100,000s USD), though moderate ongoing annual costs of up to 40% of the initial capital investment. This does not include central facility medical gas piping costs.
- Advantages: high purity, high volumes (relative to space)
- Disadvantages: requires supply chain to ASU, requires large space for safety, requires power for safety features, inefficient if low demand, require special considerations for extreme climates
References
- WHO-UNICEF technical specifications and guidance for oxygen therapy devices. Geneva: World Health Organization and the United Nations Children’s Fund (UNICEF), 2019 (WHO medical device technical series). License: CC BY-NC-SA 3.0 IGO
- Technical specifications for Pressure Swing Adsorption (PSA) Oxygen Plants: Interim guidance. Geneva: World Health Organization, 2020. License: CC BY-NC-SA 3.0 IGO
- Castle, W. F. “Air separation and liquefaction: Recent developments and prospects for the beginning of the new millennium”. International Journal of Refrigeration. 25: 158–172. January 2002 doi:10.1016/S0140-7007(01)00003-2
- PATH-CHAI Oxygen Generation and Storage, July 2021
- WHO technical consultation on oxygen access scale-up for COVID-19. WHO CC-BY-NC-SA, July 2021
- Oxygen sources and distribution for COVID19 treatment centres. WHO, April 2020
- Technical specifications for pressure swing adsorption (PSA) oxygen plants. WHO, January 2020
- Technical specifications for oxygen concentrators. WHO, September 2015
- Foundations of Medical oxygen Systems, WHO, February 2023
- Meeting Targets and Maintaining Epidemic Control (EpiC). Planning guide: Setting up liquid oxygen (LOX) systems in hospitals in low- and middle-income countries. Durham (NC): FHI 360; 2023.
Cite this post as: Sky Vanderburg, Michael Lipnick, MD, Robert Neighbour, Cornelius Sendagire, MMed. Overview of oxygen sources. OpenCriticalCare.org. Published on 15/08/2024. Accessed 04/04/2026. Available at OpenCriticalCare.org/encyclopedia/overview-of-oxygen-sources.




