

Overview of oxygen delivery devices
Contributors: Michael Lipnick, MD, Cornelius Sendagire, MMed, Rich Kallet, MS, RRT, FAARC, Rich Branson, MS, RRT, Rebecca Silvers, BSN, MSN, DnP
Date last updated: Feb 28, 2023
This article describes different types of non-invasive oxygen delivery devices including indications for use, how to setup and titrate devices, and how to choose between different device types. Complete discussions for several devices, including non-invasive positive pressure ventilation (NIPPV) and mechanical ventilation can be found separately.
Here we divide oxygen delivery devices by the amount of flow delivered to the patient:
- “Low flow delivery devices” – deliver flows <20 L/min to the patient
- “High flow delivery devices” – deliver flows >20 L/min to the patient
Illustrations of oxygen delivery devices can be found in our Creative Commons Image Library, and more information on oxygen delivery devices can be found in our O2 FAQ.
Created by the OpenCriticalCare.org Project for the WHO SARI Toolkit, 2021 CC SA-BY-NC
LOW FLOW DELIVERY DEVICES
Here we discuss low flow oxygen delivery devices as devices with flows <20 L/min to the patient. Below are also algorithms, job aids and order sets for oxygen escalation therapy in adults , pediatrics and neonates.
Most oxygen titration algorithms start with the simplest, low flow delivery device – nasal cannula. However, it is important to note that depending on locally available resources and the specific needs of the individualized patient, algorithms and selection of appropriate devices must be tailored to the local context.
Estimating oxygen concentration delivered by low flow O2 delivery devices
At RR ~20 and tidal volume ~500
20 LPM = ~0.6 FiO2
30 LPM = ~0.7 FiO2
40 LPM = 0.8 FiO2 (Farias et al)
The values represent estimates of FiO2. Actual FiO2 delivered is dependent on multiple factors including oxygen supply quality and patients minute ventilation. One general estimation rule is using oxygen flow rate: FiO2 =0.21 + 0.03 x oxygen flow rate in L/min (Frat et al). This table originally appeared at COVIDprotocols.org CC SA BY NC.



Low Flow Nasal Cannula
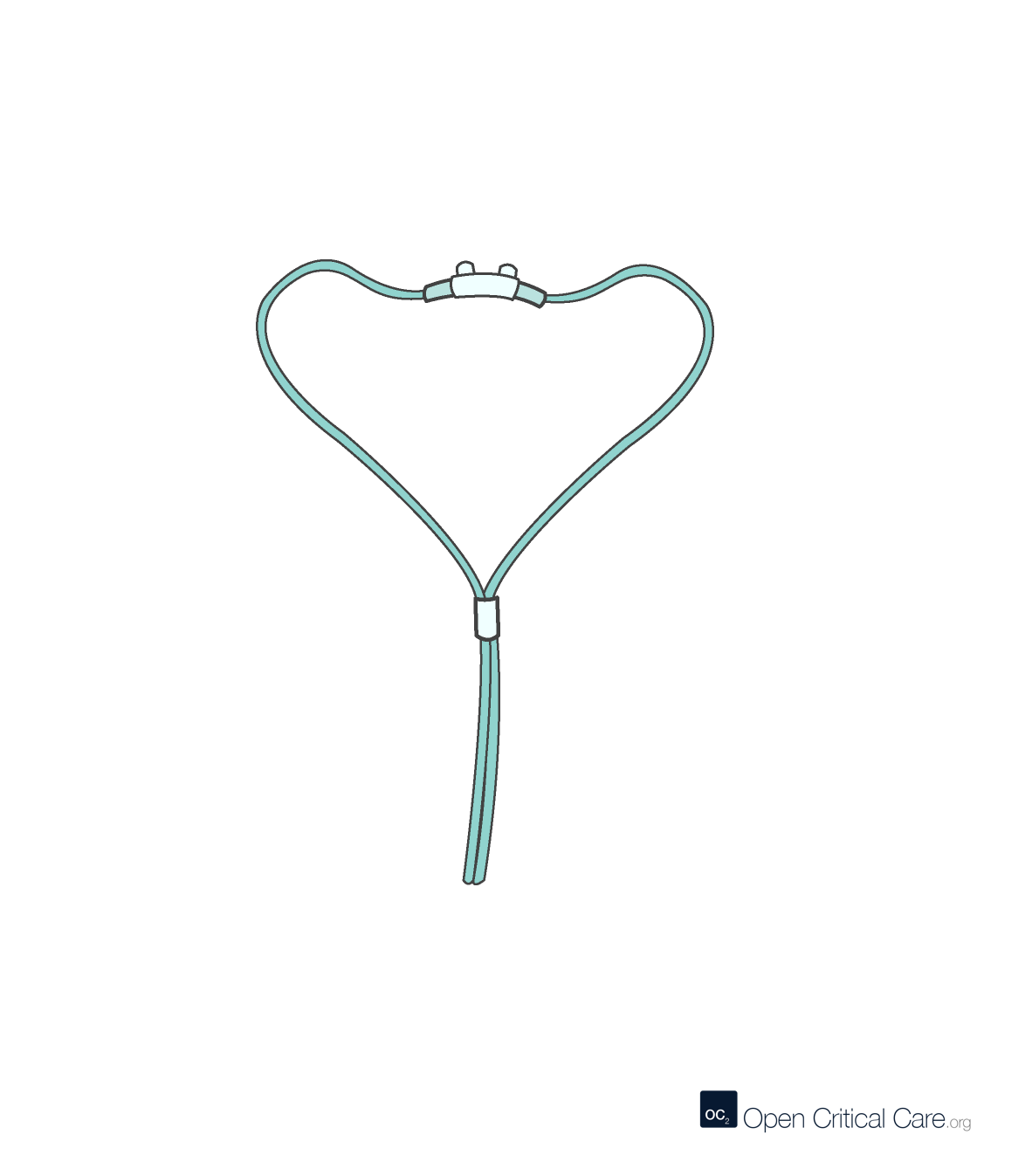
Low Flow Nasal Cannula
- O2 Flows: 0.5-6 LPM
- FiO2: 0.21-0.45 (~2-4% per LPM, variable depending on patient’s tidal volumes and respiratory rate)
- Patient population: all ages, with appropriate size interface
- Advantages: Easy to use, found everywhere and relatively inexpensive; can be used with any O2 source; no risk of gastric distension
- Disadvantages: not intended for reuse, can be uncomfortable for some patients, and does not help with work of breathing
Nasal cannula (aka nasal prongs), is one of the most commonly encountered oxygen delivery devices worldwide and the preferred method for delivering oxygen to infants and children under 5 years of age with hypoxemia, according to the WHO. A nasal cannula consists of plastic tubes that end in two short tapered prongs that are placed in the nostrils. When delivering standard flow rates with this delivery method (1-6 LPM), the flow of oxygen usually does not meet the patient’s full inspiratory demand, so ambient room air mixes with the delivered oxygen.If nasal cannula are not available, there are multiple alternative oxygen delivery devices to consider as discussed below - including nasal or nasopharyngeal catheters.
Nasal cannula should be sized by patient (neonate, infant, pediatric, adult) and can be secured with a piece of tape on the cheeks near the nose to avoid displacement, which is especially problematic in younger or altered patients. Gentle adhesive tapes designed for skin must be used to prevent skin breakdown, especially in neonates. When taping on neonates, ‘omentum’ or curling the tape should be done to avoid pressing the tubing into the skin.
The FiO2 when using nasal cannula depends on the flow rate (See ‘Flowmeters‘), prong diameter in relation to nostril diameter, the patient’s size and the patient’s work of breathing (which determine tidal volume and inspiratory flow rate).
- O2 Supply Compatibility: Nasal cannulae are not designed to regulate pressure and are thus intended to receive low-pressure gas, such as that provided by the flowmeter on an oxygen concentrator, flowmeter on an oxygen wall terminal, or dial click flowmeter integrated into a cylinder regulator. Tubing connects with standard oxygen connectors such as a tapered or barbed ‘Christmas tree’ adapter.
- Size & Fit: cannula come in ~4 or more sizes – neonate, infant, pediatric and adult (different prong spacing, diameter, length and flow capacity). The prongs of the cannula should be sized to not fill the nostrils completely in order to allow ambient room air in around the prongs. Straight, curved and flare tip prongs are available. The tubing usually has 3–5 mm internal diameter and 7–8 mm external diameter, and is specially designed to be anti kink.
- Delivered O2 Concentration: 24-45% at 1-6LPM respectively in adults; Increasing the flow rate delivered through a nasal cannula increases the delivered oxygen concentration by 2-4% per liter per minute increase. The actual FiO2 will vary widely depending on the patient’s respiratory rate and tidal volume.
- O2 consumption: consumption is the liters per minute set by the user
- Single patient use.
- Indications: Patients who are hypoxemic, without significant increased work of breathing and require low to moderate FiO2 to achieve oxygenation goals.
- Special considerations: standard nasal cannula deliver flow equally through both nasal prongs. However, ‘sampling nasal cannula’ may be encountered, which are designed to deliver flow only through one of the two nasal prongs. The other nasal prong has a separate connector which is intended to be connected to a gas sampling devices (such as capnography device). High flow nasal cannula (i.e. which use up to 60LPM flow) are specially designed and cannot be interchanged with standard nasal cannula discussed here.

Pediatric and neonatal nasal cannula
For neonates, low flow nasal cannula may be administered at flows 0-1 LPM with effectively minimal or no positive pressure (<1 cmH20), or may be administered at flows of 0-3 LPM with a blender. The blender allows delivery of controlled, lower FiO2 (e.g. 0.25 – 0.4), and the higher flows may provide some positive pressure (0-3 cmH20).
Consider the following sizes and ranges for oxygen delivery via nasal cannula in neonates and pediatrics:
WHO Respiratory equipment training video – How to select the right equipment for your health facility
Simple Facemask
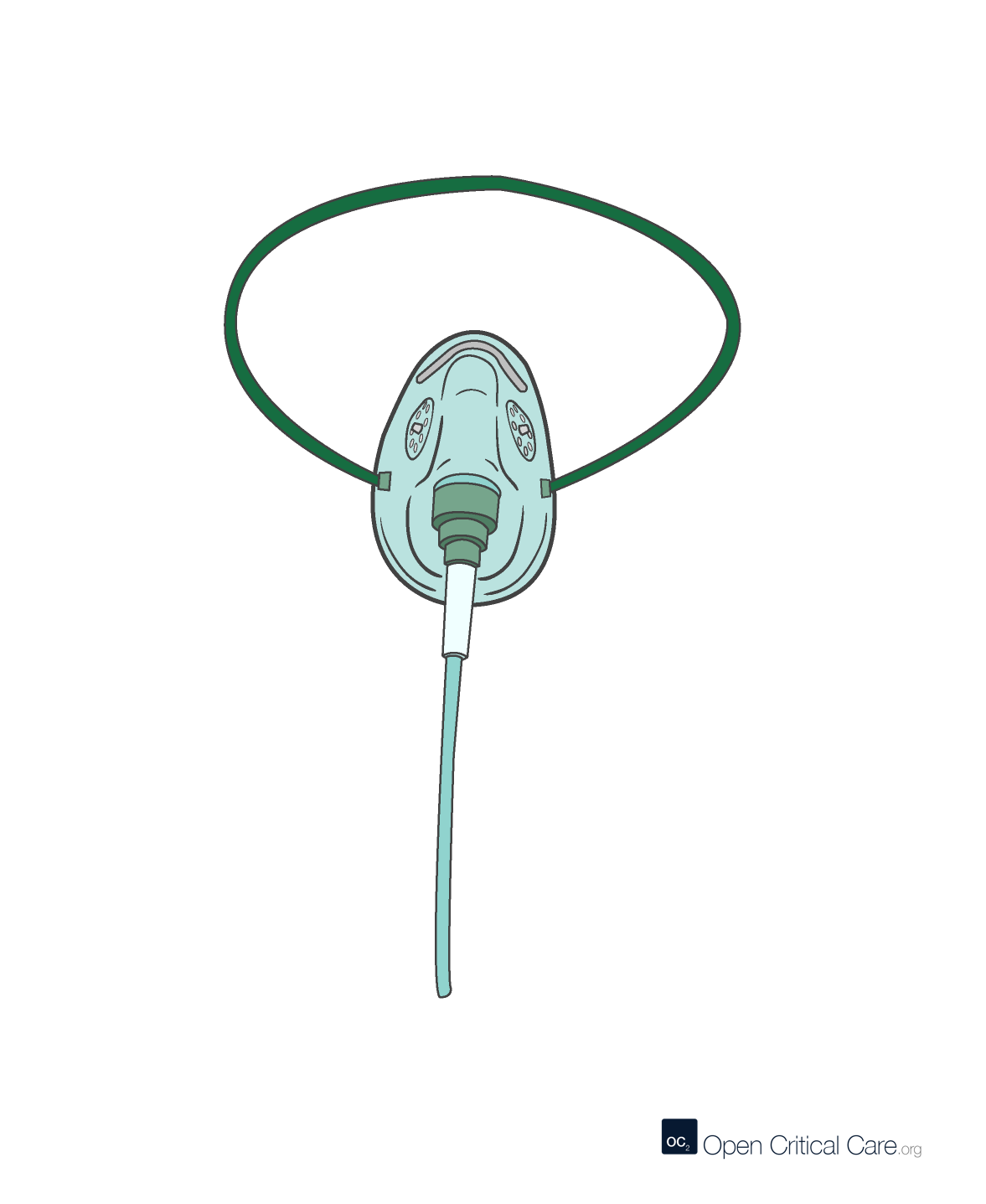
Simple Facemask
- O2 Flows 5-10 LPM (at lower flow, carbon dioxide (CO2) may accumulate in the mask)
- FiO2: 0.21-0.6 (variable depending on patient’s minute ventilation)
- Patient population: all ages, with appropriate size, though may be suboptimal for smaller pediatrics, infant and neonates
- Advantages: Easy to use, found everywhere and relatively inexpensive; can be used with any regulated O2 source, no risk of gastric distension, mask acts as a small reservoir (100-200mL) to help increase FiO2, may be better option than nasal cannula if obstruction (e.g. secretions) or epistaxis (i.e. nose bleeding)
- Disadvantages: not intended for reuse, does not help with work of breathing, can interfere with eating/drinking (especially critical for neonates, infants and pediatric patients, and can lead to rebreathing and increased work of breathing if inadequate flow
The simple facemask is a commonly encountered oxygen delivery device, not to be confused with the facemask with reservoir (also know as a non-rebreather mask). There are multiple delivery devices that may seem to function similarly to a simple facemask, but have unique considerations e.g. an oxygen tent, head box, or shovel facemask for ‘blow-by’ oxygen(NOTE: Head boxes, facemasks, incubators and tents all require high oxygen flows to avoid carbon dioxide accumulation (rebreathing), and thus can have significant associated cost and be considered wasteful. Also, head boxes and facemasks interfere with feeding, especially for neonates, infants and pediatrics. In light of these limitations, these methods are not recommended especially in settings where oxygen supplies are limited..
When delivering standard flow rates with this delivery method (5-10 LPM), the flow of oxygen usually does not meet the patient’s full inspiratory demand, so ambient room air mixes with the delivered oxygen.
Facemask should be sized by patient (neonate, infant, pediatric, adult) and are secured with an elastic strap above the ears and around the head to avoid displacement, which is especially problematic in younger or altered patients.
The FiO2 when using simple facemask depends on the flow rate, the patient’s size and the patient’s work of breathing (which determine tidal volume and inspiratory flow rate).
- O2 Supply Compatibility: Simple facemasks are not designed to regulate pressure and are thus intended to receive low-pressure gas, such as that provided by the flowmeter on an oxygen concentrator, flowmeter on an oxygen wall terminal, or dial click flowmeter integrated into a cylinder regulator. Tubing connects with standard oxygen connectors such as a tapered or barbed ‘Christmas tree’ adapter.
- Size & Fit: facemasks come in ~2 or more sizes – pediatric and adult. The larger the mask, the larger the ability for the mask to act as a small reservoir (100-200mL) to help increase FiO2. However, larger masks also contain more deadspace and may increase rebreathing and work of breathing.
- Delivered O2 Concentration: 24-50% at 5-10LPM respectively in adults
- O2 consumption: consumption is the liters per minute set by the user
- Single patient use.
- Indications: Patients who are hypoxemic, without significant increased work of breathing and require low to moderate FiO2 to achieve oxygenation goals. May be a better option than nasal cannula in patients with nasal obstruction of epistaxis (i.e. nose bleeding)
- Special considerations: simple facemask should not be confused with non-rebreather facemasks or partial rebreather facemasks as described below. Flow must be at least 5 L/min to avoid rebreathing and carbon dioxide (CO2) accumulation.
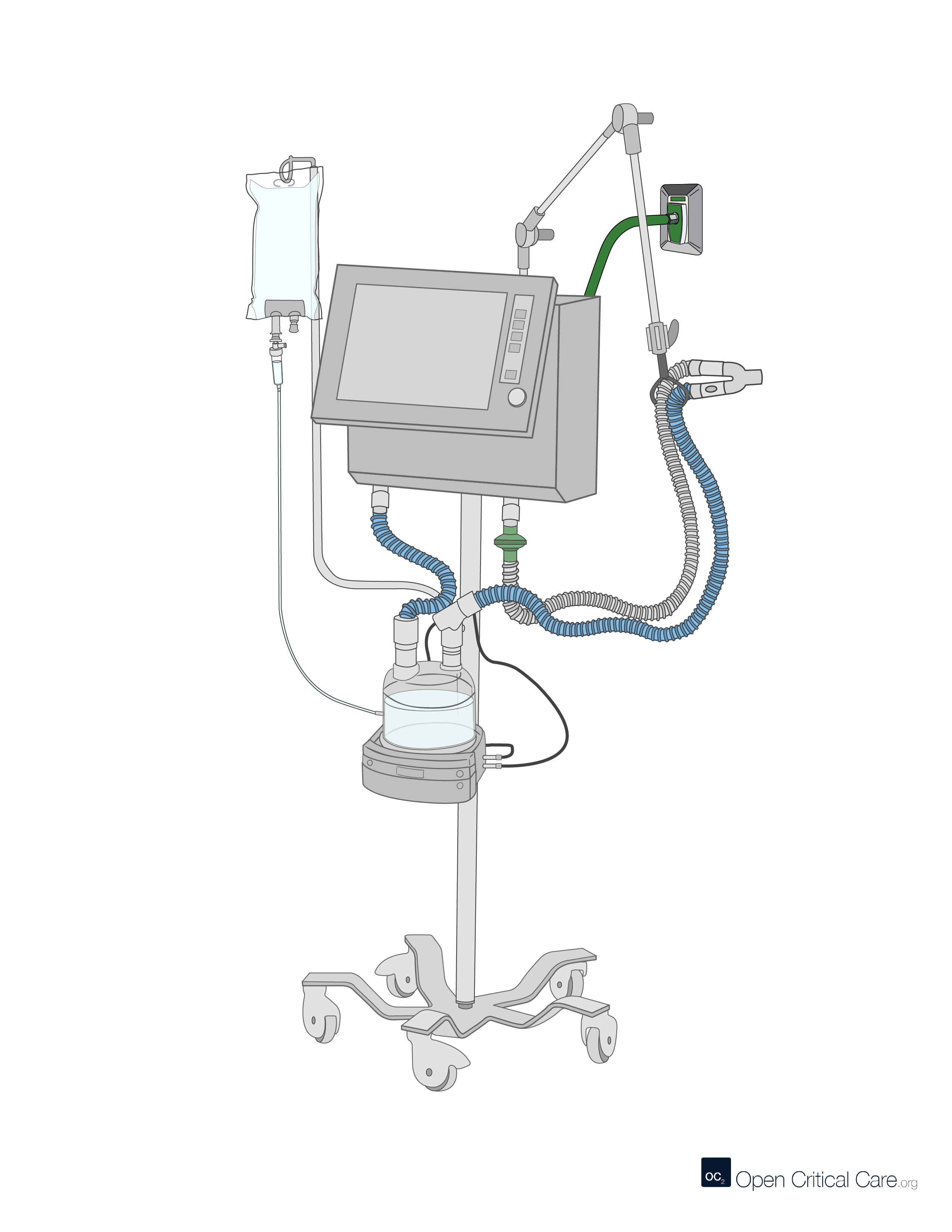
Bubble CPAP

Bubble CPAP
- O2 Flows 5-10 LPM
- FiO2: 0.21-0.6 (variable depending on patient’s minute ventilation)
- Patient population: neonates
- Advantages: Can be assembled in various low cost configurations, can be used with any regulated O2 source, provides some positive pressure in addition to supplemental O2
- Disadvantages: can be challenging to titrate and fit if never used before
Bubble CPAP devices may come in many difference configurations such as that show above, or a clinician improvised version show below. Pressure is determined by flow and the depth of the expiratory limb in the water chamber.
Titration of bubble CPAP includes:
- Start at a flow rate of 5 L/min
- Immerse the expiratory limb in the water chamber, to a depth in cm that equals the desired CPAP pressure (i.e. cmH2O)
- Look for bubbles and titrate toward 10 L/min if needed to generate bubbles
Facemask with Reservoir
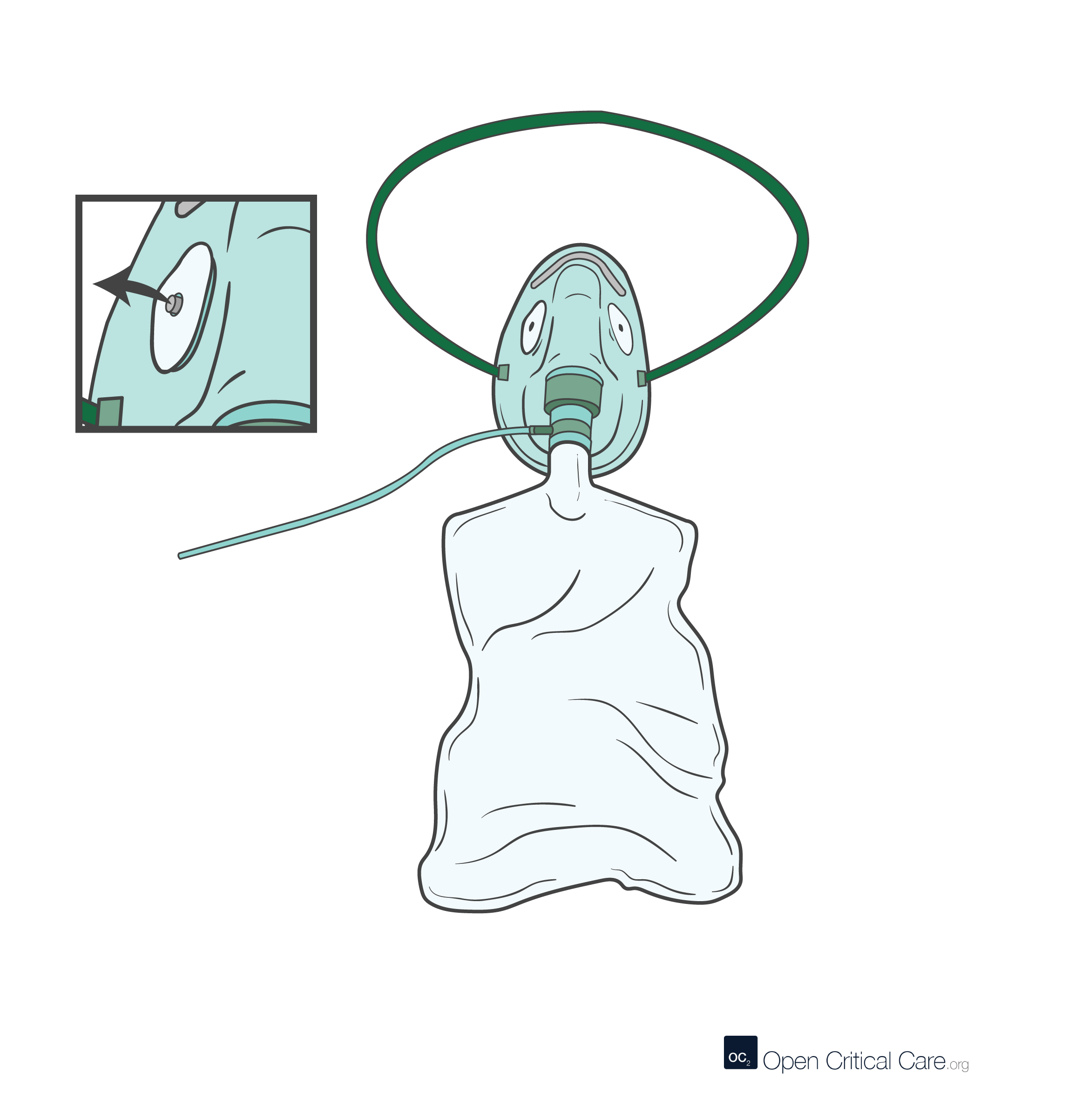
Facemask with Reservoir (non-rebreather)
- O2 Flows: 10-20 LPM
- FiO2: 0.4-0.85 (variable depending on patient’s minute ventilation)
- Patient population: Adults, though sometimes pediatric with appropriate size
- Advantages: Easy to use, found everywhere and relatively inexpensive; can be used with any O2 source capable of producing adequate flow, no risk of gastric distension, can deliver high FiO2
- Disadvantages: not intended for reuse, does not help with work of breathing, can interfere with eating/drinking, can consume significant oxygen without providing any positive airway pressure; if flow inadequate to keep reservoir inflated, then patient may get significantly less FiO2 than planned (i.e. suffocation)
The facemask with reservoir is a commonly encountered oxygen delivery device, and may come in one of two configurations:
- A non-rebreather – has a one-way valve between the reservoir bag and the facemask (to prevent exhaled breath from going into the reservoir), as well as two one-way (flutter) valves on the exhalation ports from the facemask (to prevent room air entrainment). Collectively these prevent rebreathing of exhaled breath and maximize the concentration of oxygen (FiO2) for the patient.
- A partial-rebreather – has a one-way valve between the reservoir bag and the facemask, but no one-way valves on the exhalation ports from the facemask. Thus a patient can entrain room air via the exhalation ports.
The facemask should be sized by patient and is secured with an elastic strap above the ears and around the head to avoid displacement, which is especially problematic in younger or altered patients. The relatively tight seal required can be uncomfortable for some patients, as can an oversized mask which may irritate the eyes.
The FiO2 when using a facemask with reservoir depends on the flow rate, the patient’s size and the patient’s work of breathing (which determine tidal volume and inspiratory flow rate). Flow must always be high enough to keep the reservoir inflated!
- O2 Supply Compatibility: Simple facemasks are not designed to regulate pressure and are thus intended to receive low-pressure gas, such as that provided by the flowmeter on an oxygen concentrator, flowmeter on an oxygen wall terminal, or dial click flowmeter integrated into a cylinder regulator. Tubing connects with standard oxygen connectors such as a tapered or barbed ‘Christmas tree’ adapter.
- Size & Fit: facemasks come in ~2 or more sizes – pediatric and adult.
- Delivered O2 Concentration: 50–90% at 10-20LPM respectively in adults (Note: there is considerable variation in reported measured FiO2, though rarely is 100% feasible in critically ill patients with high minute ventilation)
- O2 consumption: consumption is the liters per minute set by the user
- Single patient use.
- Indications: Patients who are hypoxemic, without significant increased work of breathing and require signifiant FiO2 to achieve oxygenation goals. Ease of setup and low cost may make this a go-to initial delivery device for critically-ill patients
- Special considerations: should not be confused with other types of facemasks described in this article
Facemask with reservoir (partial rebreather)

Facemask with reservoir (partial rebreather)
- O2 Flows: 10-20 LPM
- FiO2: 0.4-0.85 (variable depending on patient’s minute ventilation)
- Patient population: Adults, though sometimes pediatric with appropriate size
- Advantages: Easy to use and found everywhere; can be used with any O2 source capable of producing adequate flow, no risk of gastric distension, may conserve oxygen in some patients
- Disadvantages: not intended for reuse, does not help with work of breathing, can interfere with eating/drinking, can consume significant oxygen without providing any positive airway pressure; if flow inadequate to keep reservoir inflated, then patient may get significantly less FiO2 than planned; as compared to non-rebreather may deliver less FiO2 due to rebreathing
HIGH FLOW DELIVERY DEVICES
Air Entrainment Mask (i.e. Venturi mask)

Air Entrainment Mask (i.e. Venturi mask)
- O2 Flows: 4-12 LPM (entrainment flows to patient are ‘high’)
- FiO2: 0.24-0.7
- Patient population: Primarily for adults, though can be used in pediatrics if appropriate sizes available
- Advantages: can be used with any O2 source capable of producing adequate flow, no risk of gastric distension, allows user to precisely control FiO2
- Disadvantages: not intended for reuse, does not help with work of breathing, can interfere with eating/drinking, can consume significant oxygen without providing any positive airway pressure, many providers do not fully understand the purpose or use of these devices
Air-entrainment (‘Venturi’) masks can consume large quantities of oxygen relative to FiO2 delivery. They are designed to be used when precise control of FiO2 is needed (e.g. patients with dependence on hypoxemic ventilatory drive as is hypothesized as theoretically needed for some COPD patients). The table in the advanced (use slider at the top left) view of this article shows flow set on the Venturi (Air entrainment mask) – the total flow (O2 flow + air entrained) and the FIO2. This helps demonstrate why at low FIO2 – the Venturi mask provides a far more consistent FIO2 than nasal cannula or simple facemask. However, it should be noted that relatively high flows of 100% O2 are required to achieve high FiO2.
High Flow Nasal Cannula

High Flow Nasal Cannula (HFNC)
- O2 Flows: 20-70 LPM
- FiO2: 0.21-1.0
- Patient population: all ages, with appropriate size
- Advantages: Easy to use, minimal risk of gastric distension, can deliver high FiO2 and some positive pressure (1-3 cmH20 PEEP), may help avoid intubation in some patients, consistent FiO2 delivered, good humidification which can help with mucociliary clearance
- Disadvantages: not intended for reuse, can consume vast quantities of oxygen, requires specialized flowmeters, requires heated humidification, relatively expensive as compared to low flow oxygen delivery devices, usually requires intermediate pressure oxygen source (e.g. 3.4bar/55 PSI), lower and more variable positive pressure than CPAP devices
There are multiple types of high-flow nasal cannula device setups (aka high-flow nasal oxygen HFNO). All require heated humidification and a specialized patient delivery interfaces (i.e. standard low flow nasal cannula cannot be used). Some setups require considerable proprietary disposables. There are several common types of flow generator setups:
- Air oxygen blender – to mix compressed air + O2, combined with a flowmeter is the most common HFNC setup
- Venturi/port – to entrain room air via Venturi effect and mix with compressed O2; can be loud
- Turbine – oxygen and air can be supplied at low pressure
In addition to being able to provide high concentrations of oxygen and some positive pressure, HFNC also helps with deadspace washout and thus may help with work of breathing. The active heated humidification of HFNC devices can also provide greater comfort for patients as compared to a non-rebreather facemask at 10-20LPM, but also can help promote mucociliary clearance of secretions.
Titration
There are multiple strategies for titrating settings that may vary depending on the setup available. Some device setups only allow for titration of flow whereas other devices allow for titration of both flow and FiO2 (max flow depends on cannula size; up to 70 LPM for adults and 100% FiO2 ).
- Primarily flow titration strategy – the set FiO2 is fixed at 1.0 and the flow is titrated up and down based on clinical signs. Because actual FiO2 is influenced by patient inspiratory flow characteristics and minute ventilation, it may be difficult to interpret actual FiO2 or changes in clinical condition with this strategy.
- Primarily FiO2 titration strategy – the flow is fixed near the max per patient weight (e.g. ~60 LPM adults) and the FiO2 is adjusted based on clinical signs. With this strategy the set FiO2 and actual delivered FiO2 are roughly the same, allowing for easy interpretation of changes in the patient’s clinical condition (i.e. a change in SpO2 with a constant FiO2 suggests a clinical change). Additionally, by keeping flow high, this strategy maximizes the potential benefits of deadspace washout and positive pressure provided by HFNC.
High flow nasal cannula fitting & titration for neonates and pediatrics
Appropriate sizing of high flow nasal cannula is critical, especially for neonates and pediatrics. The HFNC prongs should occupy no more than 50% of the diameter of the nares to allow for flow around the cannual and to avoid excess pressure delivery.
Flow titration by weight:
- 0-10 kg 2L/kg/minute flow (max 8 LPM)
- 10-20 kg 1L/kg/minute flow
- 20-40 kg 0.5-1L/kg/minute flow (max 30 LPM)
- >40 kg 0.5-1L/kg/minute flow (max 60 LPM)
How to setup a high flow nasal cannula device
Wall or Boussignac CPAP/EPAP
Wall or Boussignac CPAP/EPAP
- O2 Flows 8-20 LPM
- FiO2: 0.5-0.85 (variable depending on patient’s minute ventilation)
- Patient population: adults
- Advantages: low cost, relatively easy to use
- Disadvantages: requires high flows of oxygen, does not provide true continuous positive airway pressure (CPAP) but rather expiratory positive airway pressure (EPAP), high flows can cause airway dryness and discomfort, limited ability to adjust FiO2
- Boussignac is a low cost, easy to use facemask CPAP-like system that has no sensors, mechanical valves or electrical components. The system connects to an oxygen flowmeter/source that generates flow dependent pressure (8LPM ~3cmH20; 15LPM ~5cmH20; 23LPM ~10cmH20)
- Traditionally used by prehospital providers for cardiogenic pulmonary edema
- In patients with hypoxemic respiratory failure (non cardiogenic pulmonary edema), it is unclear if this device would work well in patients with high minute ventilation (Sehlin et al, Resp Care, June 2011).
- There are several noteworthy potential limitations:
- Utilizes high oxygen flows
- Limited ability to adjust FiO2
- At high flows will cause airway dryness and discomfort
- No leak compensation
- No monitoring of pressures
- Provides expiratory positive airway pressure (EPAP) rather than true CPAP
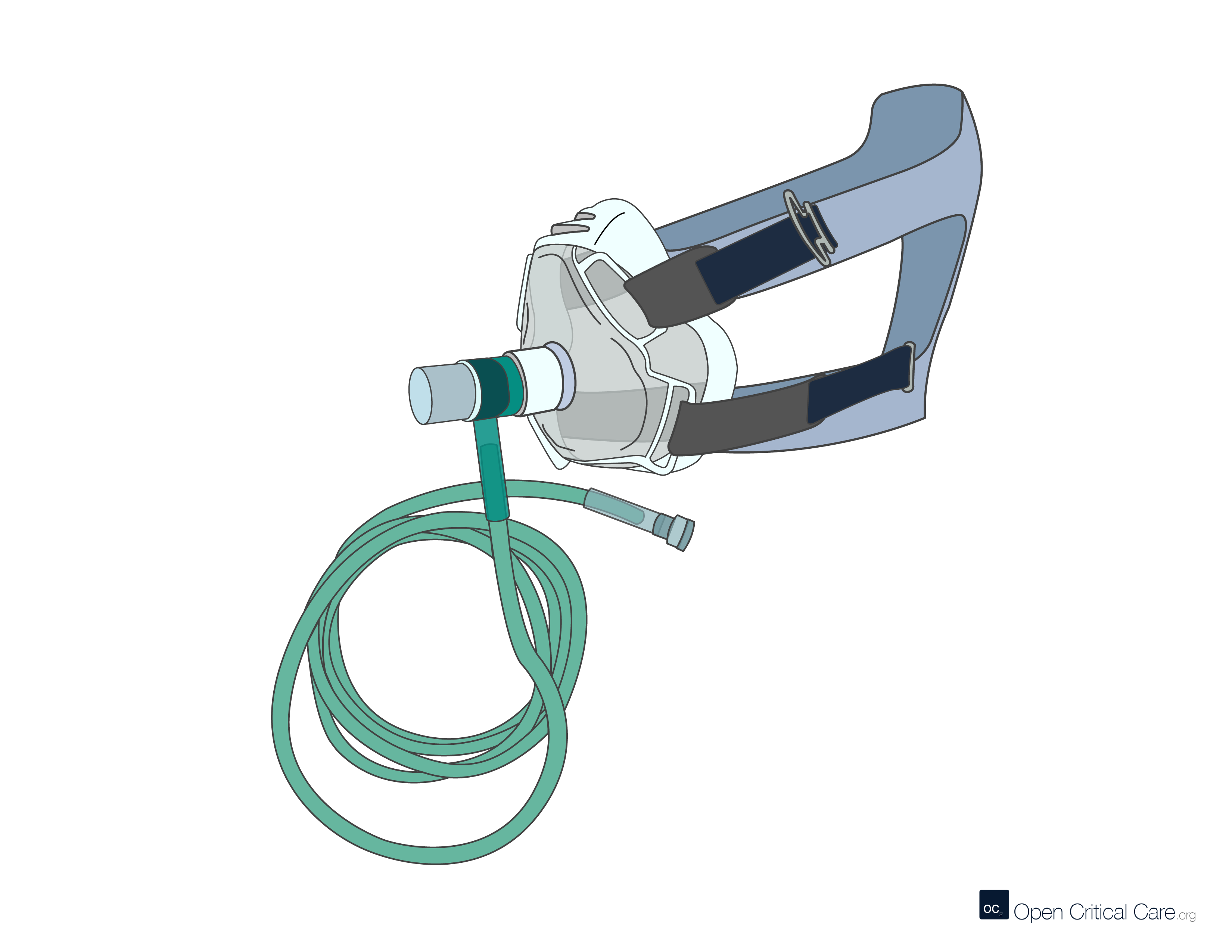
NIPPV, BIPAP, CPAP
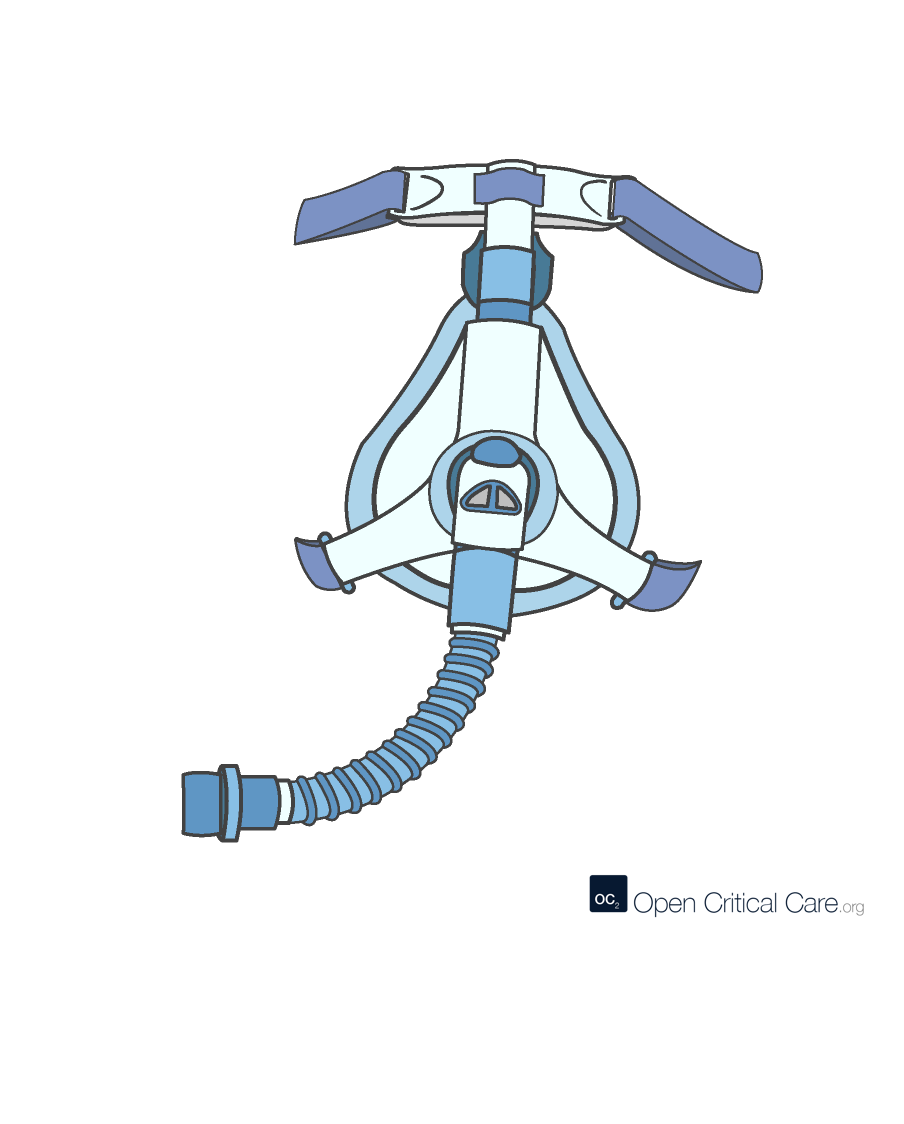
NIPPV, BIPAP, CPAP
- O2 Flows 20-100 LPM
- FiO2: 0.21-1.0
- Patient population: all ages with appropriate size interfaces and settings
- Advantages: can deliver high FiO2 and positive pressure, may prevent need for intubation in some patients
- Disadvantages: requires high flows of oxygen, can be challenging to fit and may be uncomfortable, significant misunderstanding about proper use; humidification required if used for prolonged periods.
Continuous Positive Airway Pressure (CPAP) devices or modes apply constant pressure throughout the respiratory cycle via face mask or other interface to splint open the upper airway, increase lung volume, and increase intrathoracic pressure. CPAP provides no inspiratory muscle unloading and tidal ventilation remains completely dependent on the respiratory muscles (See Figure below).
Non-invasive ventilation (NIV) or Non-invasive positive pressure ventilation (NIPPV) applies two levels of pressure during the respiratory cycle – a pressure during the inspiratory phase that is greater than the pressure applied during exhalation (See Figure below). This is effectively mechanical ventilation, and can unload the respiratory muscles and provide complete respiratory support.
Bilevel positive airway pressure (BIPAP) is a branded/trade name (by Phillips) for NIPPV/NIV as described above.
Continuous positive airway pressure (CPAP), bilevel positive airway pressure (BiPAP/NIPPV), and expiratory positive airway pressure (EPAP) waveforms comparison
(See our Full Article on NIPPV/BIPAP/CPAP or our FAQ page on NIPPV/BIPAP/CPAP)
BIPAP or Non-invasive positive airway pressure ventilation (NIPPV)
- Pros: May avoid intubation in some patients (COPD, cardiogenic pulmonary edema, upper airway obstruction) by decreasing work of breathing and adding PEEP
- Cons: Risk of infectious aerosol generation (possibly less if helmet NIPPV); risk of aspiration if patient not alert / unable to protect airway or if inspiratory pressures >20cm H2O; pt must be alert enough to remove mask if uncomfortable; skin breakdown with prolonged use; confusing terminology: IPAP (inspiratory pressure) = PS + PEEP; EPAP (expiratory pressure) = PEEP; PS of “5 over 5” is the same as PS ∆ 5 over 5, is the same as IPAP 10/EPAP 5
- O2 : requires high pressure/flow source to achieve high FiO2
- Initial Settings: PS ∆5-8/PEEP (EPAP) 5-10; titrate ∆P up to 15 to reduce inspiratory work; use higher initial IPAP with obese patients; higher pressures may require sedation in pediatric patients
Continuous Positive Airway Pressure (CPAP)
- Pros: Delivered via face mask or multiple other potential interfaces to splint open the upper airway, increase lung volume & intrathoracic pressure, prevent atelectais, overcome critical opening pressure, decrease preload and afterload which can be beneficial in volume overload
- Cons: Prolonged use is uncomfortable & causes skin breakdown; limited unloading of inspiratory muscles or provide complete respiratory support, decreased preload can have negative hemodynamic consequences in select patients
- O2 : requires high flow/pressure source to achieve high FiO2
- Initial Settings (adults/peds): CPAP or PEEP 5-10; adults: titrate as needed up to 15; peds <12; higher pressures may require sedation in peds
Evidence for non-invasive ventilation in adults
Modified from Munchsi et al, New England Journal of Medicine, November 2022
Multiple patient interfaces can be utilized to delivery NIV/NIPPV/BIPAP or CPAP.
How to setup CPAP and BIPAP
by WHO, 2021
Invasive mechanical ventilation
Invasive mechanical ventilation
- O2 Flows 20-100 LPM
- FiO2: 0.21-1.0
- Patient population: all ages with appropriate size tubing, software and modes
- Advantages: can deliver precisely controlled high FiO2 and positive pressure, can provide lung protection
- Disadvantages: requires high flows of oxygen, sedation, close monitoring, skilled staffing (including staff with ability to intubate), can cause lung injury, may be associated with high mortality especially when resources such as staff, sedation and monitoring are limited
- See complete OCC Encyclopedia article on Mechanical Ventilation
References
- Frat et al, “High-Flow Oxygen through Nasal Cannula in Acute Hypoxemic Respiratory Failure” New England Journal of Medicine. June 2015
- Munshi et al, “Noninvasive respiratory support for adults with acute respiratory failure,” N Engl J Med 2022; 387:1688-1698
Cite this post as: Michael Lipnick, MD, Cornelius Sendagire, MMed, Rich Kallet, MS, RRT, FAARC, Rich Branson, MS, RRT, Rebecca Silvers, BSN, MSN, DnP. Overview of oxygen delivery devices. OpenCriticalCare.org. Published on 28/02/2023. Accessed 28/07/2026. Available at OpenCriticalCare.org/encyclopedia/overview-of-oxygen-delivery-devices.




