

Overview of oxygen delivery devices
Contributors: Michael Lipnick, MD, Cornelius Sendagire, MMed, Rich Kallet, MS, RRT, FAARC, Rich Branson, MS, RRT, Rebecca Silvers, BSN, MSN, DnP
Date last updated: Feb 28, 2023
This article describes different types of non-invasive oxygen delivery devices including indications for use, how to setup and titrate devices, and how to choose between different device types. Complete discussions for several devices, including non-invasive positive pressure ventilation (NIPPV) and mechanical ventilation can be found separately.
Here we divide oxygen delivery devices by the amount of flow delivered to the patient:
- “Low flow delivery devices” – deliver flows <20 L/min to the patient
- “High flow delivery devices” – deliver flows >20 L/min to the patient
Illustrations of oxygen delivery devices can be found in our Creative Commons Image Library, and more information on oxygen delivery devices can be found in our O2 FAQ.
Created by the OpenCriticalCare.org Project for the WHO SARI Toolkit, 2021 CC SA-BY-NC
LOW FLOW DELIVERY DEVICES
Here we discuss low flow oxygen delivery devices as devices with flows <20 L/min to the patient. Below are also algorithms, job aids and order sets for oxygen escalation therapy in adults , pediatrics and neonates.
Most oxygen titration algorithms start with the simplest, low flow delivery device – nasal cannula. However, it is important to note that depending on locally available resources and the specific needs of the individualized patient, algorithms and selection of appropriate devices must be tailored to the local context.


Low Flow Nasal Cannula
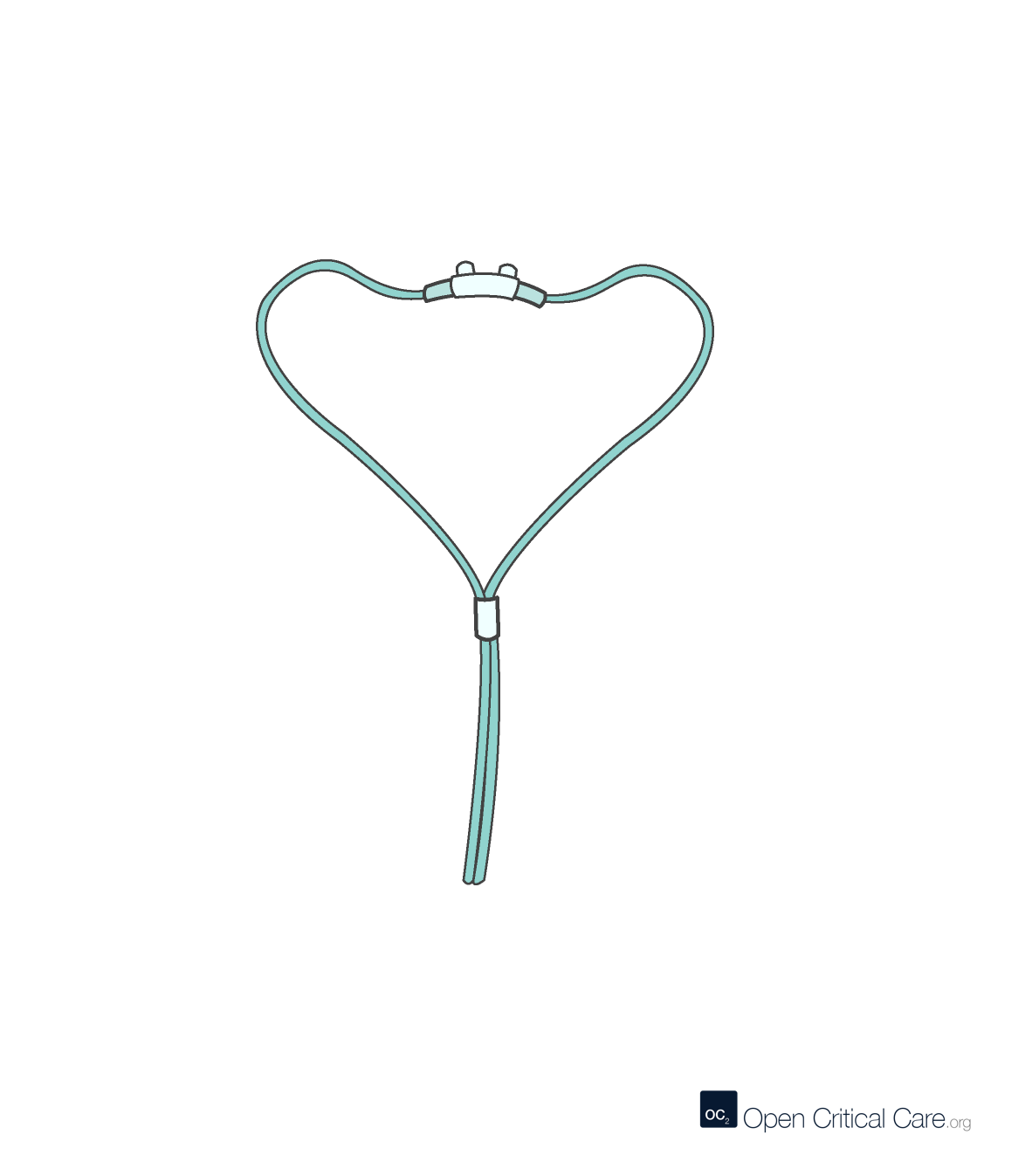
Low Flow Nasal Cannula
- O2 Flows: 0.5-6 LPM
- FiO2: 0.21-0.45 (~2-4% per LPM, variable depending on patient’s tidal volumes and respiratory rate)
- Patient population: all ages, with appropriate size interface
- Advantages: Easy to use, found everywhere and relatively inexpensive; can be used with any O2 source; no risk of gastric distension
- Disadvantages: not intended for reuse, can be uncomfortable for some patients, and does not help with work of breathing
Simple Facemask
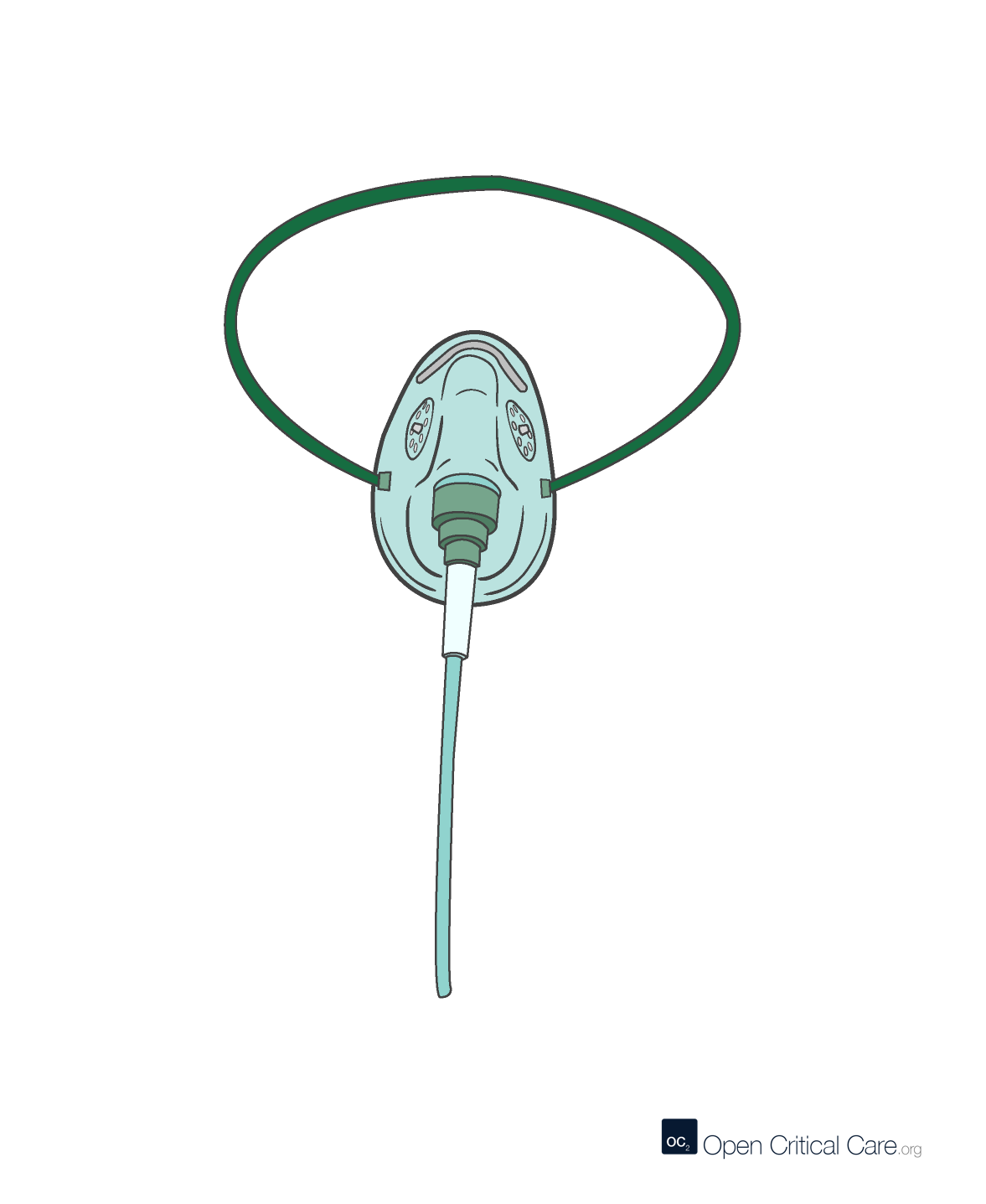
Simple Facemask
- O2 Flows 5-10 LPM (at lower flow, carbon dioxide (CO2) may accumulate in the mask)
- FiO2: 0.21-0.6 (variable depending on patient’s minute ventilation)
- Patient population: all ages, with appropriate size, though may be suboptimal for smaller pediatrics, infant and neonates
- Advantages: Easy to use, found everywhere and relatively inexpensive; can be used with any regulated O2 source, no risk of gastric distension, mask acts as a small reservoir (100-200mL) to help increase FiO2, may be better option than nasal cannula if obstruction (e.g. secretions) or epistaxis (i.e. nose bleeding)
- Disadvantages: not intended for reuse, does not help with work of breathing, can interfere with eating/drinking (especially critical for neonates, infants and pediatric patients, and can lead to rebreathing and increased work of breathing if inadequate flow
Bubble CPAP

Bubble CPAP
- O2 Flows 5-10 LPM
- FiO2: 0.21-0.6 (variable depending on patient’s minute ventilation)
- Patient population: neonates
- Advantages: Can be assembled in various low cost configurations, can be used with any regulated O2 source, provides some positive pressure in addition to supplemental O2
- Disadvantages: can be challenging to titrate and fit if never used before
Facemask with Reservoir
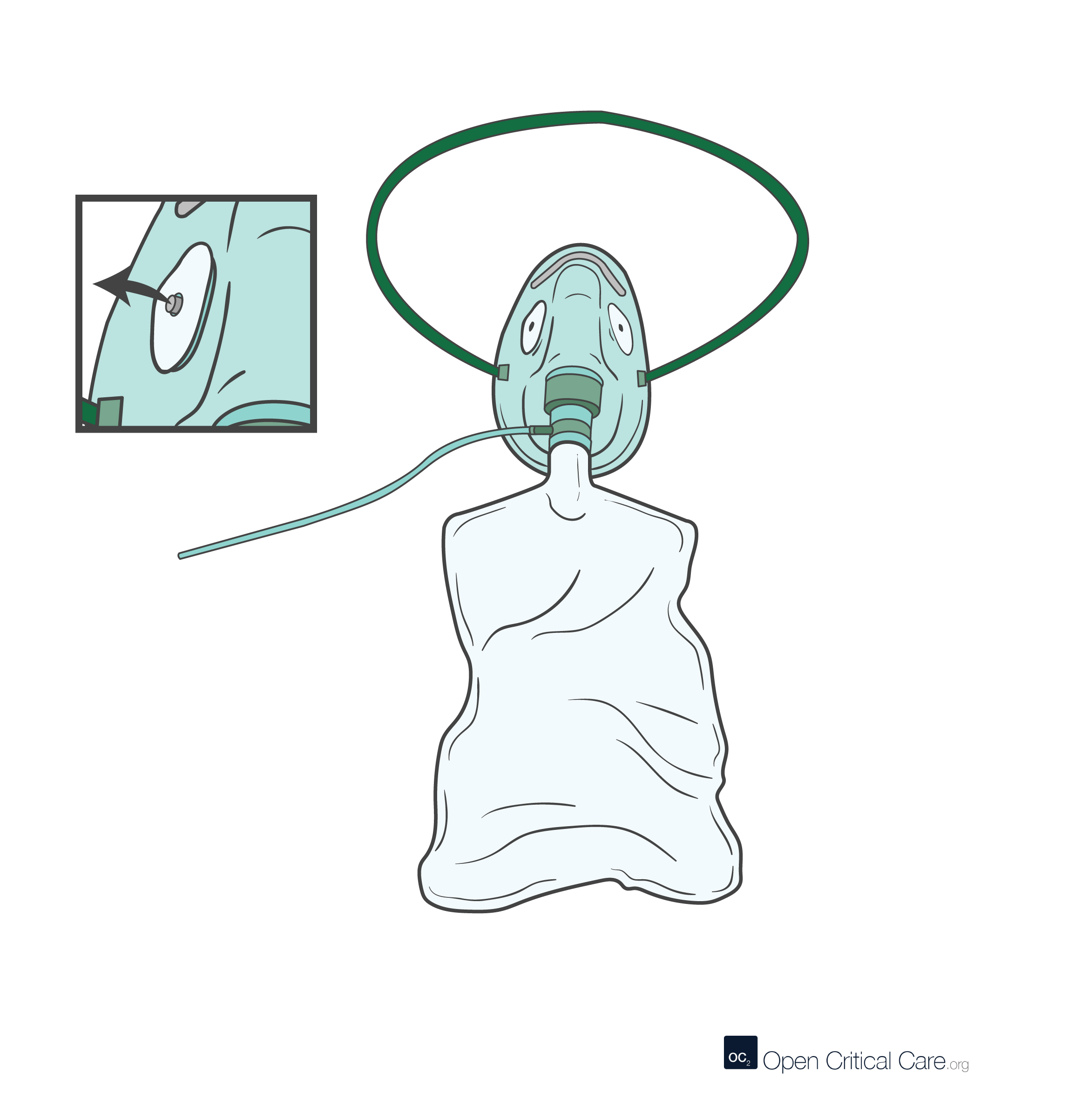
Facemask with Reservoir (non-rebreather)
- O2 Flows: 10-20 LPM
- FiO2: 0.4-0.85 (variable depending on patient’s minute ventilation)
- Patient population: Adults, though sometimes pediatric with appropriate size
- Advantages: Easy to use, found everywhere and relatively inexpensive; can be used with any O2 source capable of producing adequate flow, no risk of gastric distension, can deliver high FiO2
- Disadvantages: not intended for reuse, does not help with work of breathing, can interfere with eating/drinking, can consume significant oxygen without providing any positive airway pressure; if flow inadequate to keep reservoir inflated, then patient may get significantly less FiO2 than planned (i.e. suffocation)
Facemask with reservoir (partial rebreather)

Facemask with reservoir (partial rebreather)
- O2 Flows: 10-20 LPM
- FiO2: 0.4-0.85 (variable depending on patient’s minute ventilation)
- Patient population: Adults, though sometimes pediatric with appropriate size
- Advantages: Easy to use and found everywhere; can be used with any O2 source capable of producing adequate flow, no risk of gastric distension, may conserve oxygen in some patients
- Disadvantages: not intended for reuse, does not help with work of breathing, can interfere with eating/drinking, can consume significant oxygen without providing any positive airway pressure; if flow inadequate to keep reservoir inflated, then patient may get significantly less FiO2 than planned; as compared to non-rebreather may deliver less FiO2 due to rebreathing
HIGH FLOW DELIVERY DEVICES
Air Entrainment Mask (i.e. Venturi mask)

Air Entrainment Mask (i.e. Venturi mask)
- O2 Flows: 4-12 LPM (entrainment flows to patient are ‘high’)
- FiO2: 0.24-0.7
- Patient population: Primarily for adults, though can be used in pediatrics if appropriate sizes available
- Advantages: can be used with any O2 source capable of producing adequate flow, no risk of gastric distension, allows user to precisely control FiO2
- Disadvantages: not intended for reuse, does not help with work of breathing, can interfere with eating/drinking, can consume significant oxygen without providing any positive airway pressure, many providers do not fully understand the purpose or use of these devices
High Flow Nasal Cannula

High Flow Nasal Cannula (HFNC)
- O2 Flows: 20-70 LPM
- FiO2: 0.21-1.0
- Patient population: all ages, with appropriate size
- Advantages: Easy to use, minimal risk of gastric distension, can deliver high FiO2 and some positive pressure (1-3 cmH20 PEEP), may help avoid intubation in some patients, consistent FiO2 delivered, good humidification which can help with mucociliary clearance
- Disadvantages: not intended for reuse, can consume vast quantities of oxygen, requires specialized flowmeters, requires heated humidification, relatively expensive as compared to low flow oxygen delivery devices, usually requires intermediate pressure oxygen source (e.g. 3.4bar/55 PSI), lower and more variable positive pressure than CPAP devices
Wall or Boussignac CPAP/EPAP
Wall or Boussignac CPAP/EPAP
- O2 Flows 8-20 LPM
- FiO2: 0.5-0.85 (variable depending on patient’s minute ventilation)
- Patient population: adults
- Advantages: low cost, relatively easy to use
- Disadvantages: requires high flows of oxygen, does not provide true continuous positive airway pressure (CPAP) but rather expiratory positive airway pressure (EPAP), high flows can cause airway dryness and discomfort, limited ability to adjust FiO2
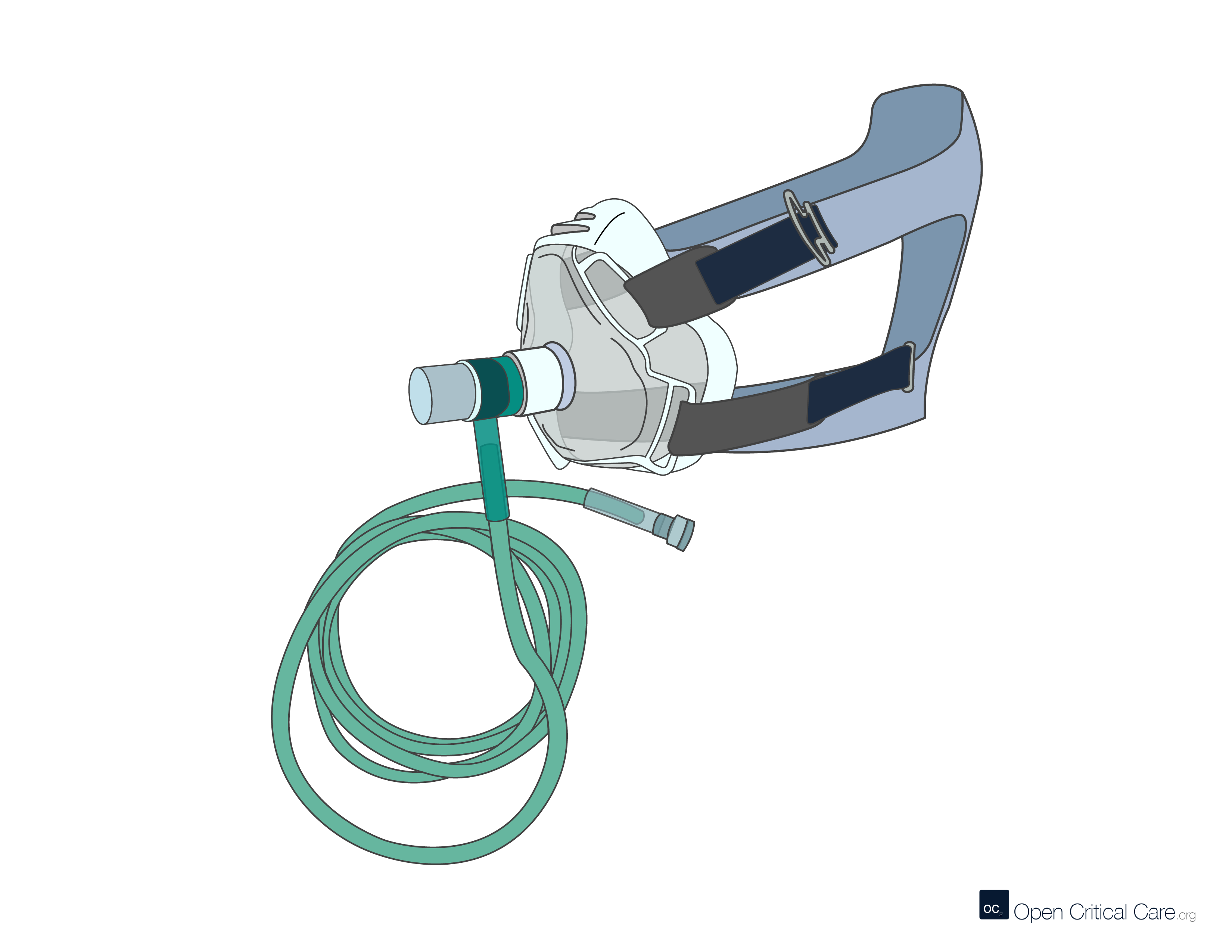
NIPPV, BIPAP, CPAP
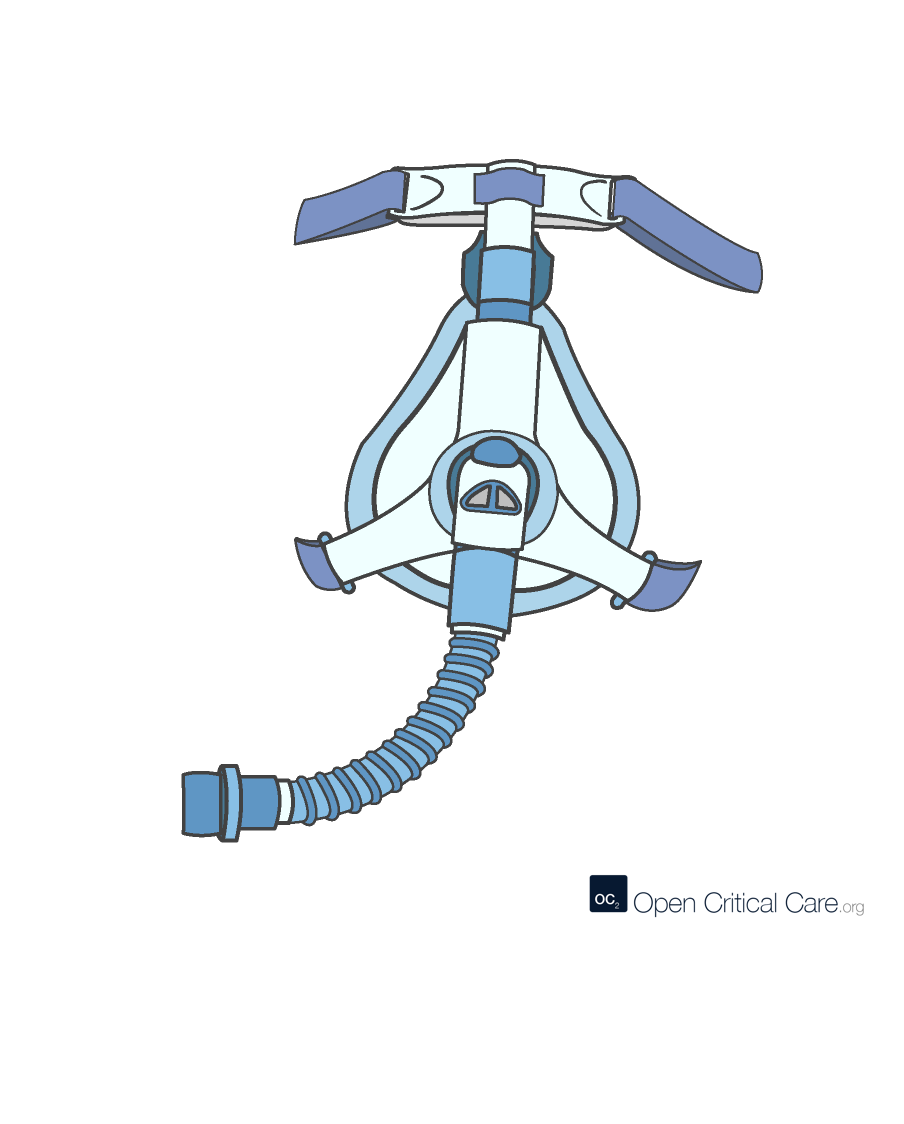
NIPPV, BIPAP, CPAP
- O2 Flows 20-100 LPM
- FiO2: 0.21-1.0
- Patient population: all ages with appropriate size interfaces and settings
- Advantages: can deliver high FiO2 and positive pressure, may prevent need for intubation in some patients
- Disadvantages: requires high flows of oxygen, can be challenging to fit and may be uncomfortable, significant misunderstanding about proper use; humidification required if used for prolonged periods.
Invasive mechanical ventilation
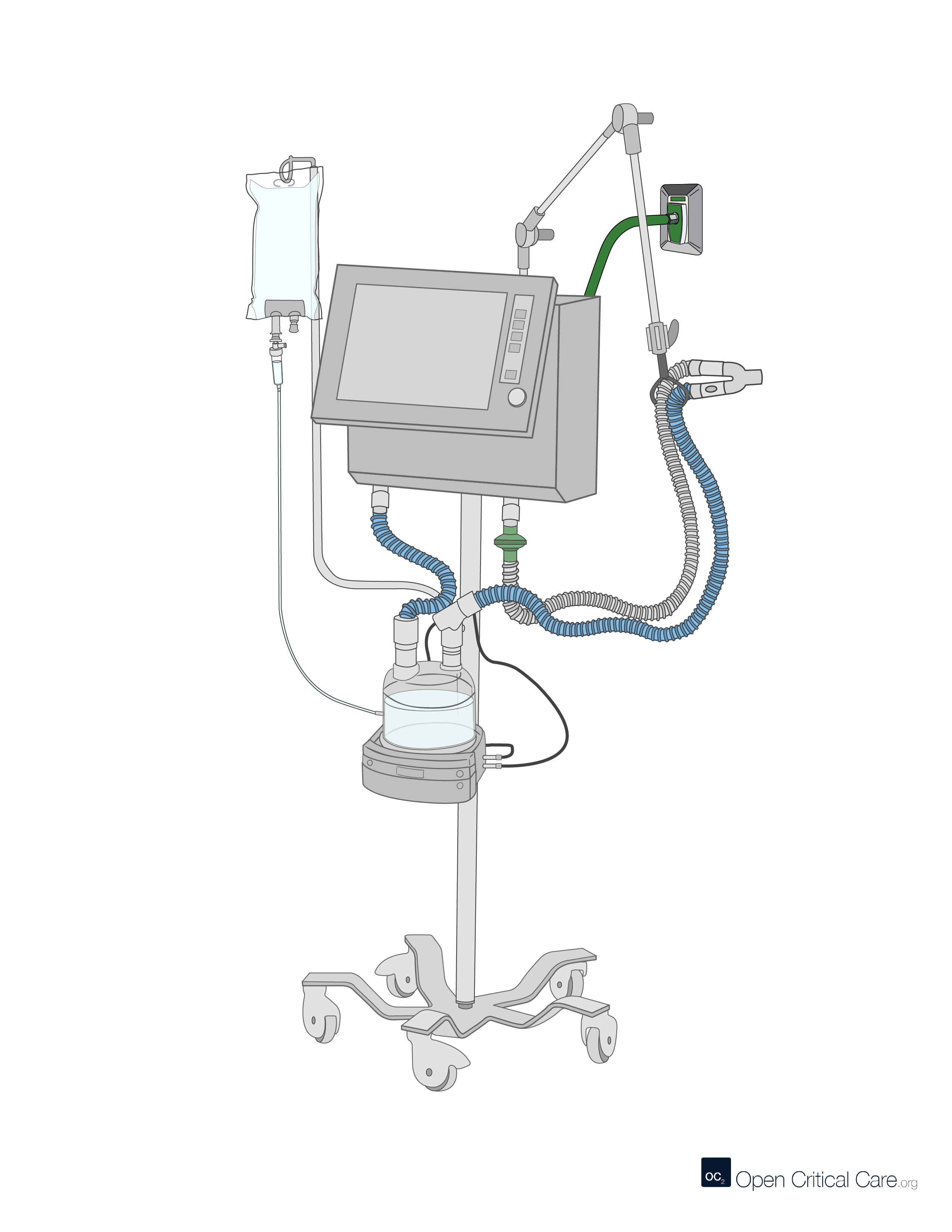
Invasive mechanical ventilation
- O2 Flows 20-100 LPM
- FiO2: 0.21-1.0
- Patient population: all ages with appropriate size tubing, software and modes
- Advantages: can deliver precisely controlled high FiO2 and positive pressure, can provide lung protection
- Disadvantages: requires high flows of oxygen, sedation, close monitoring, skilled staffing (including staff with ability to intubate), can cause lung injury, may be associated with high mortality especially when resources such as staff, sedation and monitoring are limited
- See complete OCC Encyclopedia article on Mechanical Ventilation
References
- Frat et al, “High-Flow Oxygen through Nasal Cannula in Acute Hypoxemic Respiratory Failure” New England Journal of Medicine. June 2015
- Munshi et al, “Noninvasive respiratory support for adults with acute respiratory failure,” N Engl J Med 2022; 387:1688-1698
Cite this post as: Michael Lipnick, MD, Cornelius Sendagire, MMed, Rich Kallet, MS, RRT, FAARC, Rich Branson, MS, RRT, Rebecca Silvers, BSN, MSN, DnP. Overview of oxygen delivery devices. OpenCriticalCare.org. Published on 28/02/2023. Accessed 08/04/2026. Available at OpenCriticalCare.org/encyclopedia/overview-of-oxygen-delivery-devices.




