
Oxygen FAQ
Up to date, expert answers to frequently asked questions (FAQ) about oxygen supply systems, respiratory care and pulse oximetry written by OCC & collaborators.
PSA plant
Solar is a very good power option. PV = photovoltaic – refers to the parameters by which solar panels harness electricity. Electricity is a major cost in PSA systems, so if it’s free, oxygen is essentially free. However, there are so many factors involved in solar design: latitude, how much sun you have, irradiance, cloud cover – it’s hard to generalize. In many parts of the world, including India and much of Africa, we see solar systems with batteries that have a 3-year payback. Problem is lack of funding.
Some of the challenges/considerations that need to be made when using solar options include:
Size: You need to know the size needed. E.g., if your generator requires 12 kW, solar should be sized 60kW to take care of the needs of the entire system. Solar power does not work 24 hours, depending on where you are, so you need to consider this.
Area: For a 280 LPM system, electricity requirements are 20 kW, and require 120 kW with solar, and 12000 sq foot area. Managing area is a big challenge. If you can manage to allocate a 6000 square-foot area, you can maybe install solar in this area so that at least 50% of energy will be through solar means. There are also companies that can provide space to help. Electricity boards allow you to generate electricity in one place, and you can manage the electricity where you need it. The availability of this set up varies state by state.
Investment: Solar can be costly, but there are companies in India giving solar with a 15-year contract and fixed unit charges. In Bombay and Delhi – electricity rates average 9-10 rupees per unit, but with solar you can achieve 6, 6.5 rupees/unit – so it’s cheaper.
If you are using solar then it should be 5 times the actual electricity requirement of a generator.
FAQ by Assist International
Yes, they can and often do, this is not a problem. A PSA plant should be designed and built according to an assessment of how much oxygen is needed to supply a direct pipe system plus how much oxygen should be produced to fill cylinders, simultaneously.
FAQ by Assist International
PSA plants need to be operated and maintained safely just like any other industrial motor and machinery, but they are not inherently explosive or combustible. The electrical system must be installed properly and safely. However, oxygen is an accelerant for combustion (fire). So, if there is an open flame or ignition source, an enriched oxygen atmosphere can highly accelerate fire. If oxygen is being exhausted even around the plant, there should be no ignition sources, no open flame, no smoking, no sparks allowed. If high pressure oxygen cylinders are being filled, there are additional safety considerations. NOTE: Electricity requirements are pertaining to the model and specification of each individual PSA plant, this specification must be provided by the PSA manufacturer.
FAQ by Assist International
How do I know how much oxygen my facility is using?
There are multiple strategies to quantify oxygen consumption and need for a facility. The optimal strategy may vary by facility size, oxygen source and intended use of the data. Below are several potential strategies for quantifying oxygen consumption broken down by supply side and demand side approaches.
Of note, if using data to forecast oxygen needs, plan for surges, or expand facility capacity, then current oxygen consumption may grossly underestimate optimal consumption (i.e. you must also account for patients and potential patients who currently do not have access to oxygen due to inadequate current supply).
Supply side indicators:
Measuring facility oxygen consumption may (in some settings) be most accurately done by measuring production of oxygen at the facility source. This may not always be feasible depending on the availability of special equipment and/or human resources to log such data.
- Cylinders – logs (including number, pressure and size) of cylinders delivered to wards and/or delivered to the facility
- Portable oxygen concentrators – logs of use (hours of operation can be accessed from built in hour meter found on most units, though flow rates must be known or can be estimated)
- LOX – logs of cryogenic cylinders filled and emptied based on onsite biomed logs or LOX provider delivery logs; Log of changes in mass of LOX cryogenic storage tank contents may also be available
- Oxygen PSA Plants – monitoring output of PSA plants may depend on how the plant is used – i.e. filling cylinders (in which a cylinder log may be most useful) vs directly supplying a reservoir and/or the facility via piping. Some plants may continuously display hourly flow rate of output which may be logged onsite. An alternative method for PSA plants that directly supply a facility via piping is to record flow with a mass flow meter (Example of mass flow meter) which can be configured to display and save/send such data automatically or detect flow problems.
Quantifiable demand (patient) side indicators:
Quantifying oxygen consumption from the demand side can be challenging and time consuming. This may be the only option when supply side estimates are not available or when you sek to estimate consumption for specific locations within the hospital (e.g. the intensive care unit) or specific patient populations (e.g. COVID19 patients).
When measuring or estimating oxygen consumption, one must attempt to account for leak in the O2 infrastructure as a common source of underestimating oxygen demand. This may occur for many reasons including: human error (e.g. inadvertently leaving an unused flow meter on), suboptimal practice patterns (e.g. titrating to too high of an SpO2 target) or inadequate equipment or maintenance (e.g. poorly fitted regulators, cracked tubing or piping). (Top 10 ways to conserve oxygen)
- Crude modeling of oxygen consumption by patients can be done by using oxygen consumption modeling tools but yields imprecise results.
- Pragmatic primary data collection can be done by recording (at the bedside or via electronic medical record) current consumption per patient in a facility. This includes oxygen delivery device type and settings. While total consumption will vary throughout each day for each patient and thus for the facility as a whole, it may be practical to sample such data once per day or less to obtain snapshots of facility oxygen consumption (Oxygen quantification tools compilation)
- Comprehensive primary data collection can be done daily or multiple times per day to provide the most accurate demand side estimates of oxygen consumption though require considerable resources or comprehensive EMRs.
Common pitfalls in estimating O2 consumption
- Not accounting for leak on the O2 infrastructure
- Inaccurately estimating device consumption (e.g. BIPAP/CPAP leak, ventilator bias flow etc)
- Not accounting for increased flow demand due to decreased oxygen concentration (i.e. a cylinder filled by a low quality supply or a PSA being outstripped of capacity or that is poorly maintained may produced FiO2 that is much lower than expected and thus users may attempt to improve persistent hypoxemia in a patient by increasing flow. Thus, flow consumption may overestimate true demand)
- Estimating only current consumption and not accounting for future increases and decreases in need
Long story short: If you have an oxygen plant that can fill and produce 32 cubic meters per hour, can expect 100-120 cylinders (42L) to be filled in a 24-hour period. Manufacturer gives you rate of capacity if operating every minute, every hour. Assume 80% in real life. Plants are also rated at 1000ft above sea level or lower – much of Sub Saharan Africa is above this so have to derate the plants significantly.
Also, need to consider what size of cylinder you are using – too small, too large cylinders not good – middle is where you get best economy and life span.
Additional details for understanding these conversions:
Cylinder sizes are commonly referred to by volume of liquid (water) such as 42 Liters. Then you must covert the liquid liter size to gas volume. For example, a cylinder that is 42 Liters (liquid) actually contains 6.287 (or round to 6.3) CM of oxygen in a gas state, when the cylinder is filled under pressure to 152 Bar (or 2200 psi).
PSA Plants are built to a specification that identifies a “rated” capacity of production. For example, the plant is rated to produce 16 Cubic Meters per hour. Therefore, you may calculate that 24 hour in a day X 16CM Per hr. = 384CM per day. Once the total CM per day is understood you can divide by the common size of cylinder to know how many cylinders of a given size can be produced per hr or per day. However, it is not likely that the plant will operate every minute of every hour, therefore it is reasonable to assume 80%-90% of the rated capacity will be the actual working capacity. When a PSA plant is ordered, the manufacturer will need to know the location where the plant is to be installed to design the plant with consideration to altitude above sea level, and environmental common temperature range.
FAQ by Assist International
Add the local cost of human resources of plant managers, operators, laborers and security and the operational cost of grid power and/or diesel fuel for the backup generator to the other costs of a 200 LPM capacity plant. The other costs of the 200 LPM oxygen plant cost with cylinder filling capacity will vary by vendor but estimate $200,000 USD. Time to order, deliver and install is approximately 4-6 months depending on the vendor and the supply chain efficiency. Maintenance of spare parts is estimated at $12,000 -$15,000 USD per year, plus service contract at local price. Added cost of infrastructure support for power supply, backup generator power supply, shipping, taxes, and installation cost is based on location and local costs.
FAQ by Assist International
Ventilators without a turbine or compressor generally require both high pressure oxygen (green) and high pressure air (yellow) input to function appropriately, and cannot function at all without at least one of these
Ventilators with a turbine or compressor have the ability to entrain room air directly without a compressed air source; and have variable gas inputs depending on the manufacturer, including the ability to have some combination of:
- low pressure oxygen (e.g. from a portable concentrator), via common smooth bore oxygen tubing (this may require a reservoir to augment FiO2 and an adapter to connect to the device)
- high pressure (55psi/4bar) oxygen (from central pipes or a cylinder)
- high pressure air (usually not, as the turbine or compressor provides this)
Liquid oxygen is generally more expensive than PSA due to the cost of equipment procurement, infrastructure to support the management, and distribution. After the initial investment for a very large-scale LMO production and distribution system, however, the cost will be diminished over time. LOX, LMO
FAQ by Assist International
First recall the weight of atomic and molecular oxygen: O = 15.99 g/mol and O2 = 32 g/mol
Use the ideal gas law: PV = nRT
P = pressure (in atm); V = volume (in Liters); n = amount of substance (in moles); R = ideal gas constant = 0.0821 (units are (Liters*atm)/(Kelvin*n) ); T = absolute temperature (in Kelvin)
To get the gaseous volume of 1 mole of gas: V=nRT/P
(1 mol)(0.0821 L/atm/K/mol)(273K)/1atm = 22.4 L gas
1 mole gas (STP) = 22.4L = 32g of O2
(32g/mol)(1L/22.4L/mol)= 1.428 g O2 per gaseous liter at STP
Standard temperature and pressure is 1 atm and 273K or O C
If we assume a ‘room temperature’ of 22 degrees C, then:
V=nRT/P
(1 mol)(0.0821 L/atm/K/mol)(295K)/1atm = 24.2 L gas
(32g/mol)(1L/24.2 L/mol) = 1.322 g of O2 per gaseous liter at 22 degrees C
So if you have 1000 L of gaseous oxygen: 1.322 g/L (1000L) = 1.32 kg
The primary consideration should be to ensure that the oxygen system is dependable and sustainable. The best main supply source of oxygen to a patient is a direct piped system that connects to the patient bedside from a PSA plant (or oxygen reservoir supplied by a liquid oxygen source). The direct pipe system is highly recommended and preferred. The alternative is to bring cylinders to the bedside. The back-up supply source for a direct pipe system would be a manifold of cylinders and additional spare cylinders to adequately supply the pipe system if the main supply is temporarily not operating.
FAQ by Assist International
There could be many reasons for this. If it is connected to the pipe network, it is possible the design of the pipe was not done correctly. Under “Supplementary Resources”, there are recommendations posted about rational use of oxygen that can provide further detail.
FAQ by Assist International
It depends on many local factors. Consider the materials used locally, how dusty the area is, and how hot the area is. Generally, we prefer to use masonry block and concrete for the walls and concrete floor. For the roof, consider factors such as tropical storm frequency in the area. If the area is subject to tropical storms with high winds, then consider a concrete roof. Also consider thermal mass and/or insulation of roof to minimize heat transmission.
PSA plants are much more expensive if provided in a container (also the time to build is longer). The advantage is ease of installation without a building, but a support building will be needed to manage cylinders that are being filled and the manifold for the cylinder supply (primary supply or backup supply) to a pipe system.
FAQ by Assist International
PSA is the acronym for “Pressure Swing Adsorption”, which is the name of the process that takes place inside the Oxygen Generator Plant. PSA plants extract oxygen using a molecular sieve, which expels nitrogen and leaves a more purified oxygen product, which is stored in a tank until ready for distribution by a pipe system. The basic technologies of the PSA plant include: the air (feed) compressor, the air dryer, prefilter systems, the PSA generator, and the booster compressor. Review the Assist International webinar “Essential Considerations Related to a PSA Plant” HERE for more details. You may have also heard of “VPSA” – “Vacuum Pressure Swing Adsorption”. For a detailed explanation on VPSA see: https://www.trimechindia.com/blog/oxygen-plants-whats-difference-psa-vpsa-oxygen-plant/
FAQ by Assist International
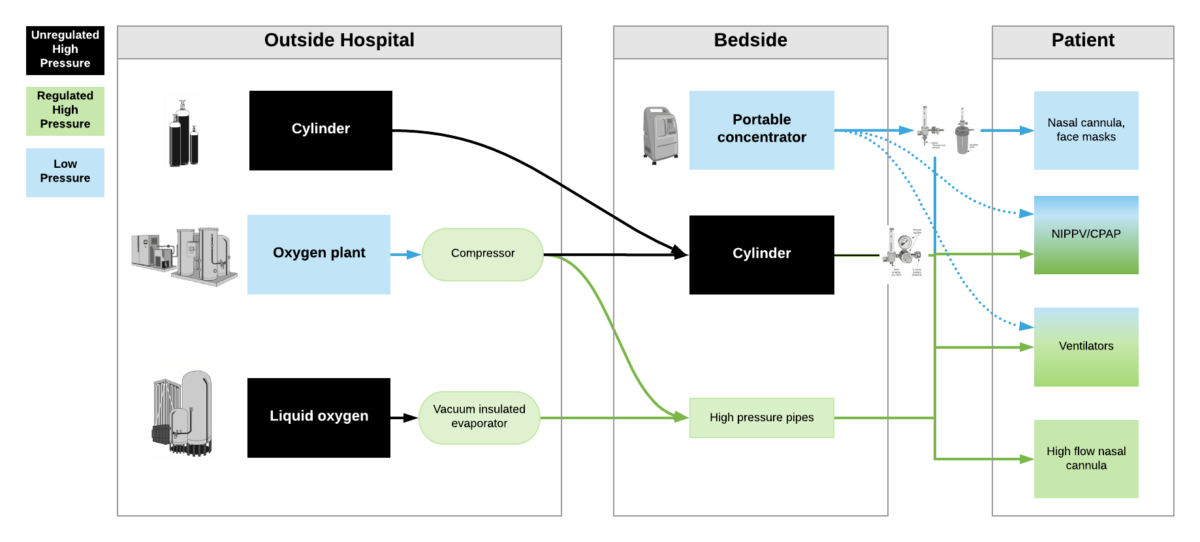
High pressure oxygen sources are capable of delivering oxygen at ~50psi/4bar to a device. These include oxygen cylinders (via regulator), oxygen plants via a compressor, liquid oxygen (via vacuum insulated evaporators) and very few portable oxygen concentrators (via additional compressor). High pressure oxygen is required for most ventilators, high flow nasal cannula and non-invasive positive pressure ventilators when taking care of critically ill patients.
Low pressure oxygen sources deliver oxygen at far less than <50psi/4bar. These include oxygen from a low flow flowmeter or a portable oxygen concentrator. Generally, these cannot deliver high enough oxygen concentrations to take care of severely hypoxemic patients.
***Some ventilators (e.g. LTV2200, Zoll 731) can operate with either high pressure or low pressure oxygen input. Other ventilators (e.g. PB560) may only be capable of utilizing a low pressure oxygen input. Of note – when utilizing low pressure oxygen input, some ventilators may not be able to provide high enough concentrations of oxygen to care for critically ill patients. Check manufacturers’ reports for maximum oxygen concentration delivery.
The first exhaust system directly exhausts the large compressor. The second exhaust would exhaust the room and make sure the room has good air circulation and the temperature is moderated. Also, sometimes the air dryer needs exhaust.
FAQ by Assist International
For staff qualifications, first determine if the staff is expected to simply operate the plant or if the staff is also expected to provide maintenance-service for the plant.
If the staff is expected to simply operate the plant, then the minimum qualification of the should be 1 staff that is a certified/qualified electrical, mechanical, or biomedical technician, plus if cylinders are to be filled, then add staff of 1 or 2 basic laborers to handle cylinders (the number of added laborers needed will depends on the number of cylinders to manage).
If the staff is expected to perform basic and/or advanced maintenance/service to the PSA plant then a certified electrical, mechanical, or biomedical engineer should be added to the staff.
The total number of staff to be hired should be based on the plan of operational hours of the plant. For example, a PSA plant is typically planned to operate for 24 hours per day, 7 days per week, therefore the total number of staff to be hired should be planned accordingly.
Initial Basic Training for PSA plant technicians and engineers is recommended to begin at the time of plant installation and commissioning by the manufacturer’s installation team. The manufacture should provide complete instruction regarding how to operate the plant, monitor, understand and record the proper performance parameters of the plant, instruction of simple and routine maintenance for the plant according to manufacturer’s specification, basic trouble-shooting, and standard operating procedures for acquiring support for service and maintenance when needed.
Advanced levels of service should only be performed by competent trained engineers and technicians, and this usually means that an “outside” service contract will be required to provide the advance levels of service that will be needed. Overall, the availability of advanced level training for PSA services is scarce and will require the PSA owner to prioritize and finance efforts to locate training opportunities to increase the knowledge, skill and abilities of their own technicians and engineers.
FAQ by Assist International